
About the Department of Health

About the Department of Health
We help Victorians to stay healthy and safe, and deliver a world-class healthcare system that leads to better health outcomes for all Victorians.

Grants and programs
Our grants and programs support health sector organisations and individuals.
Our women's health program
To bridge the gap in women's healthcare, we are leading the delivery of a program of work to change the way women's health issues are treated.

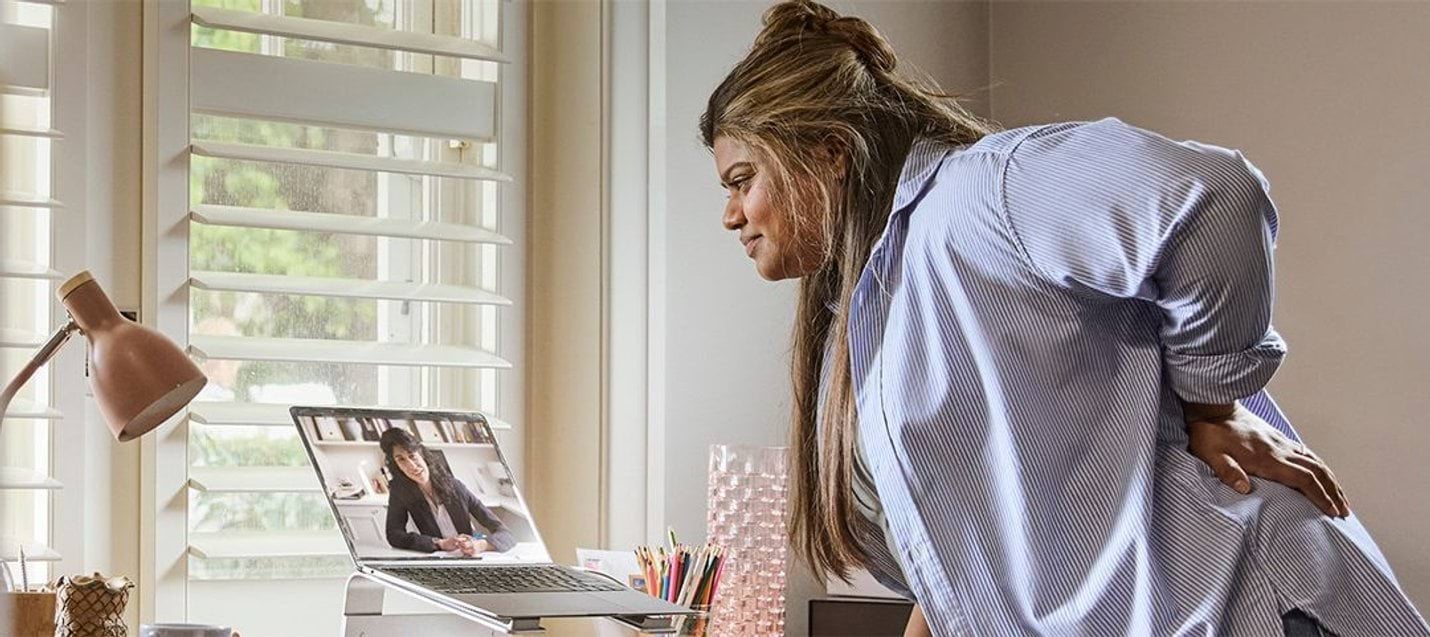
One year on: Virtual Women's Health Clinic connects more women with the care they need
The Virtual Women's Health Clinic has helped hundreds of women and girls access free healthcare in its first year of operation, connecting them with expert support and advice.

The Peer Healing Space is now open
The Peer Healing Space is a free, residential mental health service for anyone aged 18 or older experiencing high levels of distress. It provides short-term mental health support, in a home-like setting.

Victoria marks one year of Local Health Service Networks
Victoria’s Local Health Service Networks were established on 1 July 2025. They bring health services in 12 geographic regions together to plan and coordinate care around local needs.
Our key focus areas
Explore how we are supporting the health and wellbeing of Victorians.

Hospitals and health services
Models of care, quality and safety standards, funding and governance, data reporting, and system reform.

Public health
Public health policy, prevention, surveillance and emergency response, including health protection, promotion and population health systems.

Mental health and wellbeing
Services, reform, workforce, safety and quality, and integrated care across settings.
Primary and community health
Service delivery, commissioning, workforce, prevention, and integration with hospitals and social care.
Alcohol and other drugs
Alcohol and drugs services, including harm reduction, treatment and recovery, policy, commissioning and workforce initiatives.
Ageing and aged care
Residential and community care, quality and safety, workforce, funding and system reform.
Improving your health and wellbeing
Find services and programs for Victorian's on the Better Health Channel website.

Women's health and wellbeing
Women across Victoria can now access free or low-cost expert healthcare.

Don't risk the flu. Get vaccinated today.
This winter season, help protect your child from serious illness with a free flu vaccine.

Chemist Care Now
Victorians can now be treated for more conditions. Visit your local participating chemist to get the care you need.
Publications

Research and reports
Explore our research and reports.

Policies, standards and guidelines
Explore our policies, standards, manuals and guidelines.

Forms and templates
Find various forms and templates.
Information for
Updated
