

- Date:
- 21 July 2023
Safer Care Victoria has developed the toolkit as part of our Department of Health's Planned surgery recovery and reform program.
Additional health sector resources are available on our Planned Surgery Recovery and Reform SharePoint site.
For access, contact the Planned Care Recovery and Reform team via plannedcare@health.vic.gov.au.
Key principles for safe introduction and expansion of day surgery models
{kind=link}
Day surgery implementation toolkit overview
An overview of day surgery models, their benefits and the key principles to their safe introduction and expansion.
Day surgery models – also known as same-day surgery models – admit and discharge the patient the same day they have surgery. Discharge suitability should be assessed on criteria and if the patient is clinically stable post-operatively.
The benefits of day surgery models for well-selected patients include:
- supporting patient engagement in their care decisions and empowering them in their own recovery by facilitating their return to a familiar environment
- reducing risks of hospital-acquired complications
- promoting early mobilisation and faster return to baseline performance in activities of daily living.
Day surgery models also optimise use of health system resources, including:
- decreasing hospital length of stay
- improving patient flow (service wide)
- minimising hospital-initiated postponements secondary to bed blockages
- increasing theatre utilisation
- reducing surgical waitlists.
Key principles
Safer Care Victoria recommends following the key principles below for safe introduction and expansion of day surgery models. The key principles within this toolkit serve as a template for health services to use to guide safe implementation of day surgery models of care.
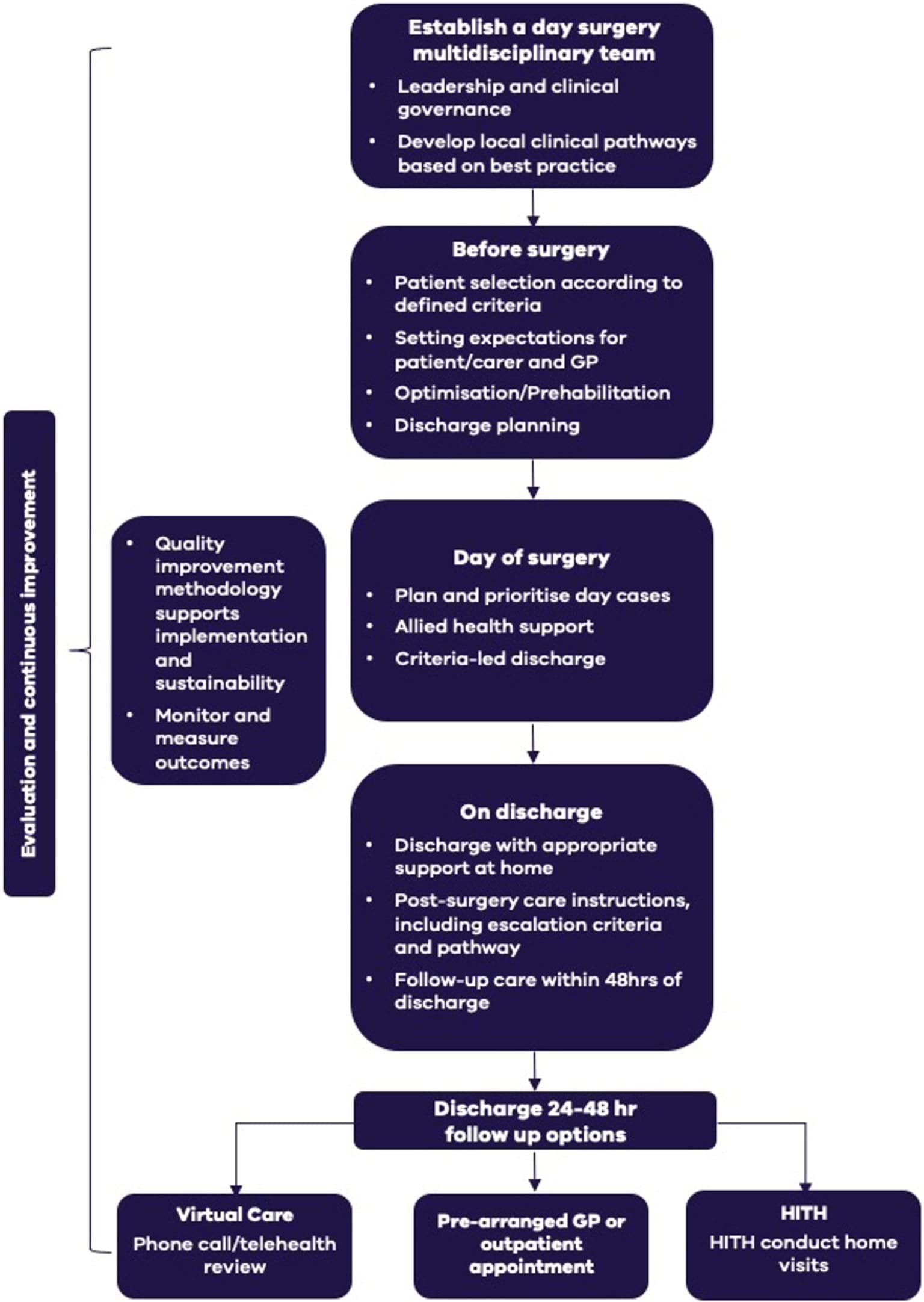
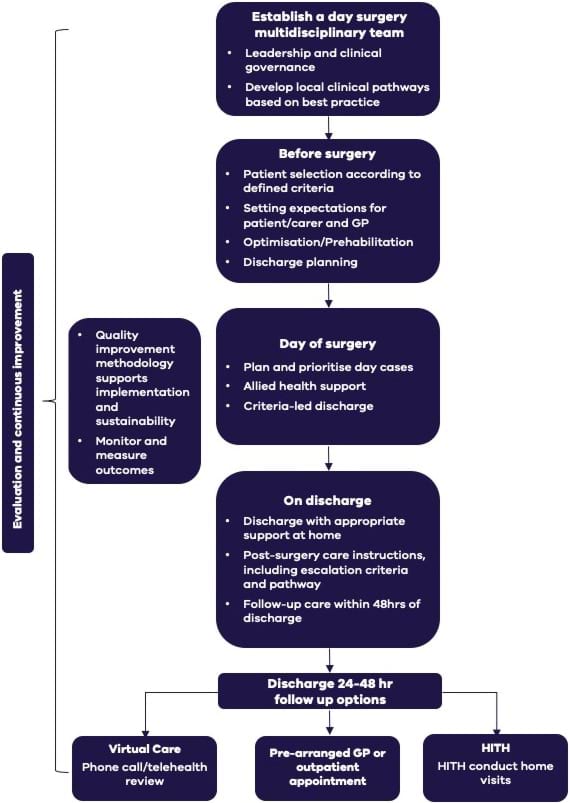
Key principles for safe introduction and expansion of day surgery models
Acknowledgements
We would like to acknowledge the New South Wales Agency for Clinical Innovation and Queensland Health for their previous work on day surgery models of care, which served as a foundation for this toolkit.
We also extend our thanks to the Safer Care Victoria (SCV) Perioperative Learning Health Network staff (LHN) and advisory group members for their invaluable contributions, and the creators of the resources featured in this toolkit. Their efforts have been instrumental in making this toolkit possible.
Establishing a multidisciplinary team
Establish a leadership and governance structure and develop local clinical pathways.
Engaging the perioperative team
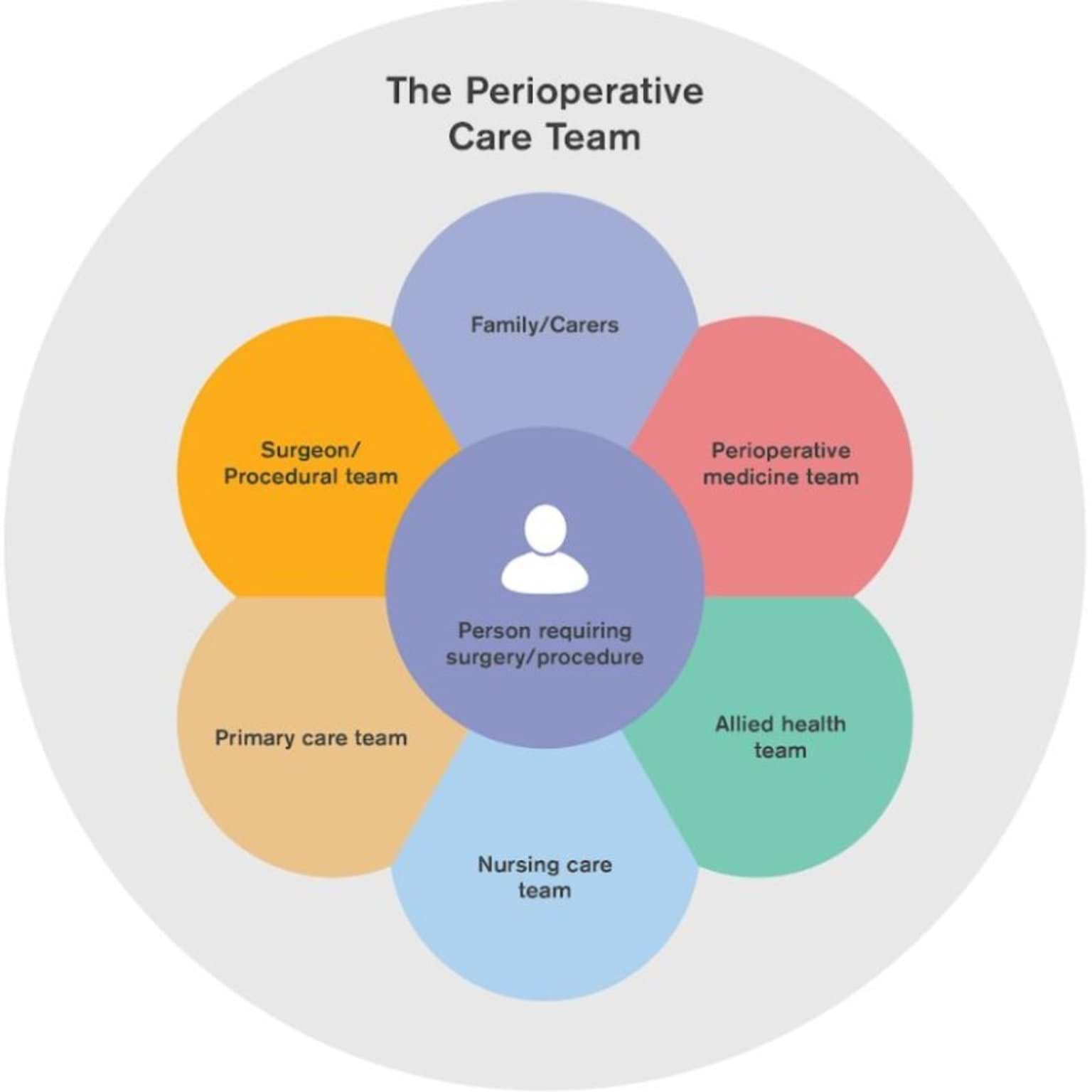
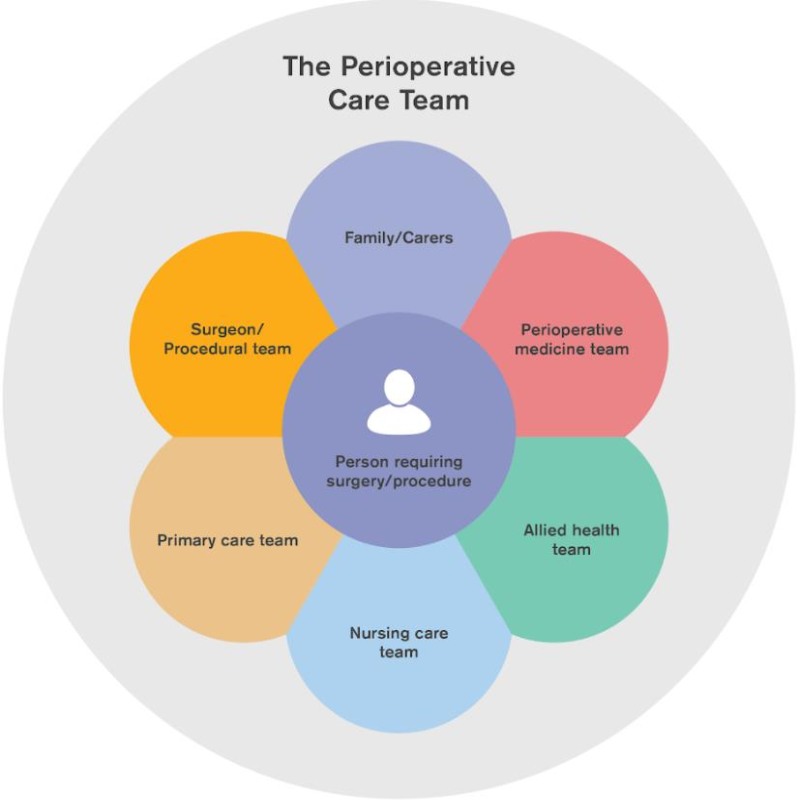
Engagement with the perioperative team (see Figure 2) across the entire surgical patient journey is important when developing best care day surgery models. Successful models require executive sponsorship and multidisciplinary team (see allied health support) involvement in developing and implementing pathways.
Implementation should be guided by an agreed project plan that is appropriately resourced. Local steering committees and working groups should be established to support day surgery programs. It is essential to identify all relevant stakeholders who may be impacted by the introduction of a day surgery model. This includes clinical and non-clinical staff and executive leadership.
Figure 2: The perioperative care team (POCT)
{kind=link}
Establishing a leadership and governance structure
Clinical governance includes all of the integrated systems, processes, leadership and culture that are central to providing safe, effective, accountable and person-centred care, underpinned by continuous improvement.
Strong executive support is crucial for developing, approving, and implementing new day surgery models of care. The role of the sponsor is to ensure project goals are aligned to broader health service strategies and to ensure appropriate project resourcing.
Clinical leaders across craft groups (who ultimately support the patient through their surgical journey) are responsible for the approval of clinical pathway development, escalation procedures and continuous monitoring for safety and quality. Regular evaluation of the model should take place, and work should be underpinned by a robust change and communication strategy accessible to all stakeholders.
The 5 domains of clinical governance are interrelated (see Figure 3) and should be considered by all health services designing and implementing new day surgery models of care. These domains can be tailored to support consumers and staff to work together to achieve high-quality care.
Figure 3: 5 domains of clinical governance

{kind=link}
“Clinical governance is essentially an organisational concept aimed at ensuring that every health organisation creates the culture, the systems and the support mechanisms so that good clinical performance will be the norm and so that quality improvement will be part and parcel of routine clinical practice.”
Sir Liam Donaldson speaking at the Conference on the Development of Surgical Competence on Clinical Performance and Priorities in the NHS, November 1999
Developing local clinical pathways
Structured care pathways for day surgery aim to enhance the coordination and continuity of clinical care. These pathways should entail a sequence of decisions and actions that should be documented to ensure clear communication among all parties involved, including the patient and caregiver.
It is important that the clinical pathways are in agreement with the patient and can be adjusted if deemed clinically necessary. The pathway should provide consistent and transparent expectations and education to the patient and caregiver, as well as regular reassessments of their suitability for the pathway or escalation of care if needed.
Ultimately, the clinical pathways or protocols will be determined by the specific procedure or surgery, guided by best practice evidence, and agreed upon by all key stakeholders, while being adaptable to meet local health service needs.
Example pathways for specific procedures exist, such as the NSW Health Joint Replacement Pathways Framework.
When developing day surgery clinical pathways, there are important considerations at each stage:
Before surgery
- Risk screening
- Pre-arrange discharge destination and follow-up plan
- Individual patient requirements
Day of surgery
- Fasting protocols
- Appropriate anaesthesia to support same-day discharge
- Clinical handover
- Escalation pathways
- Criteria for discharge/admission
On discharge
- Education requirements for patients and caregivers
- Support required on discharge
- Escalation pathway post discharge (i.e. how does the patient/caregiver/GP escalate deterioration/concern?)
- 24-hour follow-up options
- Handover to community services and primary care providers
Resources to support implementation
Before surgery
Select, optimise and prepare patients for day surgery to ensure the best possible outcomes.
Patient selection
Not one single factor alone dictates suitability for day surgery. The procedure, patient factors, and discharge destination all must be suitable for safe day surgery.
Patient selection for day surgery requires a comprehensive baseline assessment of the perioperative risk using a validated surgical risk assessment tool. Review of social factors including distance from a hospital and availability of someone to care for the patient overnight need to be considered as part of proactive surgical planning and management.
When selecting suitable patients it is important to consider the following:
Patient selection should be based on agreed inclusion and exclusion criteria developed by each individual service that takes into consideration the capability of the service providing surgery.
Resources to support implementation
Setting expectations
It is crucial to set clear expectations from the initial patient and carer interaction to alleviate anxiety and emphasise that day surgery is the norm, rather than the exception. To achieve this, the healthcare team, including the primary care practitioner, must convey a consistent message from the moment of referral for surgery. One effective way to ensure this is by creating staff question and answer scripts.
Effective communication with the primary care provider is also essential to optimise pre-surgery care and facilitate post-discharge care escalation. They must be informed of the plan for day surgery and given clear expectations of how to support their patient throughout their surgical journey.
Resources to support implementation
Patient optimisation and prehabilitation
Elements of multimodal prehabilitation

{kind=link}
Patient optimisation prior to surgery helps to ensure the best possible outcomes for patients.
Prehabilitation is a process that aims to enhance a patient’s physical and psychological function to support them before, during and after surgery.
Prehabilitation and optimisation of comorbidities pre-surgery can:
- reduce length of stay
- reduce risk of post-operative complications
- enhance recovery post surgery
- improve cardiorespiratory fitness
- improve nutritional status
- encourage the patient to quit smoking and drinking alcohol
- prepare the patient psychologically and emotionally for surgery
- improve surgical outcomes
- improve population health
- improved the patient experience.
The level and type of prehabilitation/pre-surgical care required by the individual patient depends on the surgery risk, patient risk and comorbidities.
Shared decision-making and optimisation programs need to be multimodal to help empower the patient to take control of their perioperative journey. Digitally facilitated prehabilitation is a cost-effective model that can be accessible to a large number of patients, such as via smartphone, tablet or computer. Capitalising on digitally enabled patients who are comfortable with this format for education, resource access and tracking progress can also facilitate self-management abilities.
Day of surgery
Plan and prioritise day cases, utilise allied health support, and implement criteria-led approach for safe patient discharge.
Planning and prioritising day cases
It is important to plan and schedule surgery lists to ensure day ward hours meet the needs of increased day cases.
Considerations include:
- planning for day surgery cases early on the morning theatre list
- scheduling as indicated according to recovery times for different procedures or types of patients (e.g. patients with diabetes, or who are very young or very old)
- monitoring the volume of planned surgery waiting lists and adjusting the capacity of day wards and post-operative support services to meet any increased day case demand.
Allied health support
Multidisciplinary allied health team members are vital throughout the entirety of the perioperative journey, from initial screening to discharge and post-operative care.
Allied health team members may include, but are not limited to:
- physiotherapists
- occupational therapists
- dietitians
- social workers
- speech pathologists
- pharmacists
Key allied health team members, such as a senior physiotherapist, may also be designated to a care coordinator role to facilitate the day pathway.
Roles and responsibilities of allied health team members will be agreed within the context and demands/resources of the individual health service.
Resourcing of evening allied health and nursing support is required to promote safe and successful day surgery.
Examples of allied health roles and responsibilities at different stages of the pathway are as follows.
Before surgery
- Patient assessment and education
- Safety risk assessment
- Early identification and escalation of patient concerns to surgeon
- Scheduling theatre list and arranging follow-up care
- Optimisation and prehabilitation services
- Coordination of discharge support and a follow-up care plan, including a criteria-led discharge pathway
Day of surgery
- Contact person for carer and patient
- Documentation as per local care pathways
- Monitoring and updating the follow-up care plan
On discharge
- Early identification and escalation of patient concerns to surgeon
- Patient and carer education (e.g. mobility, medications, equipment)
- Activity of daily living equipment provision as indicated
- Assessment and management for functional rehabilitation goals
- Contact person for carer and patient
- Care coordination and onward referral as indicated
Criteria-led discharge (CLD)
Introduction of CLD will help support safe discharges. CLD is a formalised discharge approach that requires the patient to meet pre-determined criteria in order to discharge when clinically and socially safe to do so.
CLD is designed to facilitate efficient processes and shared knowledge of discharge requirements among the entire multidisciplinary team. For CLD to be successful, it is essential to have a clear pathway that ward staff can follow without need for medical support.
Implementation of new CLD pathways need to be continuously reviewed to ensure implementation is effective and sustained.
It is important to use quality improvement tools to support implementation, evaluation and continuous improvement.
See also ‘use quality improvement tools to support implementation and sustainability’.
Key steps to CLD development and implementation:
- Review/develop aim, objectives and scope of implementation
- Create a governance structure
- Establish a project team and plan to ensure a sustainable approach
- Develop CLD documentation
- Educate and train staff, families and carers
- Monitor and evaluate indicators and measures
On discharge
Prepare and communicate a clear discharge plan to ensure patients have appropriate support at home.
Discharging with appropriate home support
All day surgery patients should have a clear discharge plan prior to admission to ensure they are supported through the post-operative phase of care.
This should include:
- pre-arranged transport home
- a designated carer capable of monitoring recovery and providing care
- any additional equipment or supports arranged prior to admission
- staff, carer and patient information on what post-operative complications to look out for, and how to escalate concerns
- a documented clear and structured escalation plan for patients and other health providers that meets local protocols and pathways
- appropriate discharge location and environment, including staying within 30 minutes from their nearest health service. Medihotels provide an option for those who do not have appropriate accommodation options close to a health service
- appropriately selected follow-up plan that meets patient, surgeon and resourcing needs, with contact within 24 hours of discharge. These may include virtual care, Hospital in the Home services, a pre-arranged GP appointment prior to admission, or outpatient services.
Post-surgery care instructions
It is important to communicate post-operative care instructions clearly and effectively, including the criteria for escalating any concerns.
- Clear written and verbal post-operative instructions should be provided to patients or their carer in consideration of health literacy. This includes instructions on pain management, a follow-up care plan, and clear escalation criteria.
- A phone number should be provided to the patient, carer and GP so any questions, concerns, or need for emergency advice can be addressed in a timely manner. Closed loop communication should facilitate communication back to the person escalating the concern.
- Accessibility of written and verbal information should be considered relative to the needs of the patient and/or carer in the pre-operative phase. This ensures provision of discharge support that is timely and appropriate for people who are culturally and linguistically diverse or who have higher accessibility needs in line with clinical care standards.
24-48 hour follow-up care
For safe, effective day surgery models, appropriate monitoring is required post discharge. All day surgery patients should be contacted from 24 to 48 hours post discharge.
The chosen option for follow-up will depend on local service resources/pathways, type of surgery, patient/surgeon preference and patient factors, such as age and risk.
Discharge pathways that can ensure timely follow-up within 24 hours of leaving hospital may include:
- A virtual model of care – Follow up with a phone call, text message, video call, or message through a remote patient monitoring (RPM) platform.
- Pre-arranged GP or outpatient appointment – Clearly communicate with the patient’s GP to inform them of day surgery, pre-arrange an appointment, and provide them with clear information on expectations for the primary care practitioner.
- Hospital in the Home (HITH) or Better at Home services – These services provide post-operative care in the home that would otherwise need to be delivered within a hospital as an admitted patient. HITH may also be utilised on occasions when patients require admitted care in preparation for planned surgery. Note that the patient is not eligible for GP care while at home under the HITH bed card.
Evaluation and continuous improvement
Use quality improvement tools to support implementation and sustainability.
Quality improvement tools to support implementation
Implementing new day surgery pathways requires continuous review and evaluation to ensure change improvement is achieved and sustained.
Measurement for quality improvement, benchmarking and reporting should be embedded in the perioperative process.
Safer Care Victoria has a step-by-step guide to using the Model for Improvement as the framework to guide improvement work.
The Clinical Excellence Commission in NSW also provides a range of tools and resources to help design, measure and evaluate your work.
Linking with other champion health services for mentoring support during the implementation phase can also ensure the success and sustainability of safe day surgery models.
Measuring clinical and non-clinical outcomes
Monitoring safety and quality indicators related to day surgery performance will help promote safe expansion of day surgery.
|
Measure |
Definition |
Rationale |
|---|---|---|
|
Unplanned admissions (planned day surgery cases) |
Number of patients planned as day cases who require overnight bed |
To monitor the unforeseen need for hospital beds for planned day cases. Helps to measure effective patient selection for day surgery. |
|
Unplanned readmission |
Readmission within 48 hours and 28 days post discharge from surgical admission |
Quality and safety measure. To monitor for unforeseen complications. |
|
Representations to emergency department |
Representations to the emergency department within 30 days of procedure and reason for presenting |
Quality and safety measure. To monitor for re-distribution of patients from one part of the system to another. |
|
Mortality |
Mortality at 30, 90 days and 12 months |
Quality and safety measure. |
|
Hospital-acquired complications (HAC) |
As per national HAC definitions |
Quality and safety measure. |
|
Major medical complications |
Major medical complications within 30 days (stroke, myocardial infarct, and pulmonary embolism) |
Quality and safety measure. |
|
Patient experience |
Patient survey to capture feedback on patient experience |
To evaluate how the changes have affected the patient’s experience. |
|
Proportion of potential day procedures performed as day procedures in patients with suitable selection criteria (e.g. ASA 1 and 2) reported by health service/campus. |
Number of patients who meet selection criteria to receive day surgery for the targeted procedure |
To allow comparison between suitable patients and the number of day cases being performed. |
|
Number of day cases performed for each targeted procedure |
Number of day cases performed |
To monitor the number of patients receiving day surgery. |
Procedures suitable for day surgery
A list of procedures identified as suitable for day surgery in Victoria.
This list identifies examples of suitable procedures that can be safely performed as day surgery by applying the key principles outlined in this tool kit.
It is not intended to be an all-inclusive list of procedures suitable for day surgery at all Victorian health services. It is important to always consider the capability of the individual site where the surgery is being performed.
- Anterior cervical discectomy and fusions
- Breast biopsy
- Carpal tunnel release
- ENT biopsies
- Hand procedures
- Inguinal hernia repair
- Knee procedures including arthroscopy
- Laparoscopic cholecystectomy
- Lens procedures
- Muscle, nerve and temporal artery biopsies
- Nasal procedures, fractured nose manipulation, rhinoplasty, septoplasty
- Paediatric OSA, grommets, and some middle ear/mastoid procedures
- Peripheral nerve surgery
- Skin and subcutaneous procedures/excisions
- Simple cervical decompression and foraminotomies
- Simple lumbar decompression and microdiscectomies
- Sinus procedures
- Skull tumours and other wholly intraosseous lesions
- Some shoulder procedures
- Surgical termination of pregnancy
- Tonsillectomy/adenoidectomy
- Total hip arthroplasty (THR)
- Total knee arthroplasty (TKR)
- Umbilical hernia repair
- Uni-compartmental knee replacement