

- Date:
- 25 May 2023
In these guidelines:
Introduction
This section explains the purpose of the Infection Prevention and Control Guidelines.
1.1. Purpose
These guidelines describe specific infection prevention and control (IPC) measures required to reduce the transmission of COVID-19.
It applies to health workers and care staff, infection control professionals, managers, support workers and other healthcare staff in settings such as:
- acute/subacute healthcare
- first responders and patient transport
- residential care facilities
- primary and community health care.
Many of the IPC principles in these guidelines can also be used in the community and in non-healthcare workplaces, particularly the:
- chain of infection
- hierarchy of controls
- cleaning
- hand hygiene
- respiratory and cough etiquette.
Note: Healthcare workers must refer to and always comply with their organisation’s policies and procedures.
Key messages
COVID-19 is predominately transmitted via inhalation of aerosols (both short- and long-range transmission is possible) particularly when an infected person is in close contact (<1.5m) with another person.
Transmission via direct contact with contaminated surfaces is possible but not common. Factors affecting transmission are:
- the concentration of viable virus shed in aerosols expelled by the infected person in the form of particles (ranging from respiratory droplets to smaller aerosols)
- the type of contact the infected person has with others, how close they are and whether the virus can enter via their mouth, nose, or eyes
- the characteristics of the setting of transmission and the infection prevention and control measures which are in place.
To reduce the transmission of COVID-19 in healthcare settings, it is essential to:
- understand standard and transmission-based precautions
- apply the hierarchy of controls
- manage routine care of suspected or confirmed cases of COVID-19 using personal protective equipment (PPE).
Variants of concern will continue to emerge. These guidelines give information for mitigating the risks of variants of differing levels of infectivity and transmissibility.
Treatment/care of patients and outpatients should not be denied or delayed because of COVID-19 IPC precautions.
1.2. Coronaviruses and COVID-19
Coronaviruses are a large family of viruses that cause illness of variable severity in humans. They include the common cold, severe acute respiratory syndrome coronavirus (SARS-CoV), Middle East respiratory syndrome coronavirus (MERS-CoV) and severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
SARS-CoV-2 is the virus that causes coronavirus disease 2019 (COVID-19).
1.3. Modes of transmission
The COVID-19 virus (SARS-CoV-2) is spread by exposure to respiratory fluids carrying infectious particles. The risk of exposure to respiratory particles is highest when in close contact (within 1.5 metres where the concentration of particles is highest) with an infectious person who has respiratory symptoms, for example, coughing or sneezing.
Exposure can occur in three ways:
- Airborne transmission—very small, infectious aerosol particles can stay suspended in the air for prolonged periods of time. Inhaling aerosols is the main means of transmission of COVID-19.
- Droplet transmission—droplets containing infectious particles can be inhaled or deposited on mucous membranes (mouth, nose, or eyes).
- Indirect contact transmission—droplets with infectious particles can contaminate surfaces. Touching a contaminated surface and then touching the mouth, eyes, or nose without performing hand hygiene, can expose a person to infection. Note, however, that the risk of transmission by indirect contact is low.
1.4. Symptoms
Symptoms include cough, breathing difficulty, sore throat, runny nose, or nasal congestion with or without these other symptoms:
- headache
- myalgia
- fatigue
- diarrhoea
- nausea/vomiting
Less commonly:
- loss of appetite
- loss of smell or loss of taste
- fever (≥37.5C) or history of fever; for example, night sweats, chills.
- In the elderly, consider new or increased confusion, change in baseline behaviour, falling or exacerbation of underlying chronic illness.
All people with recent onset of new or worsening symptoms of an acute respiratory infection (ARI) should be tested for COVID-19 and managed as a possible case until COVID-19 is excluded or an alternative diagnosis is confirmed. Clinical judgement should be applied where there are alternative clinical explanations for symptoms or where non-specific symptoms are present.
1.5. Incubation and infectious period
A standardised operational definition of the infectious period for COVID-19 is used for public health activities including contact identification and management. See the department's COVID-19 (Coronavirus disease 2019) advice.
1.6. Outbreak management information
Each outbreak will differ according to the circumstances of the facility or department; therefore, the investigation and management will be applied on a case-by-case basis after identification and understanding of the features of the outbreak.
To remain prepared for COVID-19 outbreaks, each facility must have an Outbreak Management Plan.
For more information, see Management of Acute Respiratory Infection Outbreaks including COVID-19 and influenza in residential care facilities.
For more information on outbreak response procedures, see the department's COVID-19 (Coronavirus disease 2019) advice.
For further advice and guidance, see Coronavirus Disease 2019 (COVID-19) CDNA National Guidelines for Public Health Units.
1.7. Review
The information in this online publication is based on evidence and national recommendations. As new evidence or resources become available, content in this online publication may be updated. Be aware that any printed copy of this publication may become outdated and should always be compared to current information in this online publication.
Principles of infection prevention and control
An overview of infection prevention and control (IPC) strategies to reduce COVID-19, based on the chain of infection and hierarchy of controls.
2.1. The chain of infection
Transmission of infectious agents requires the following elements:
- a causative agent/pathogen (for example SARS-CoV-2)
- a reservoir
- a portal of exit
- a means of transmission
- a portal of entry
- a susceptible host.
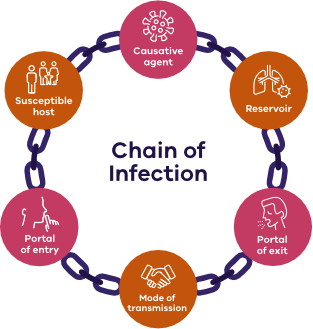
Infection prevention and control measures aim to break one or more of the links in the chain to limit or prevent the transmission of the pathogen.
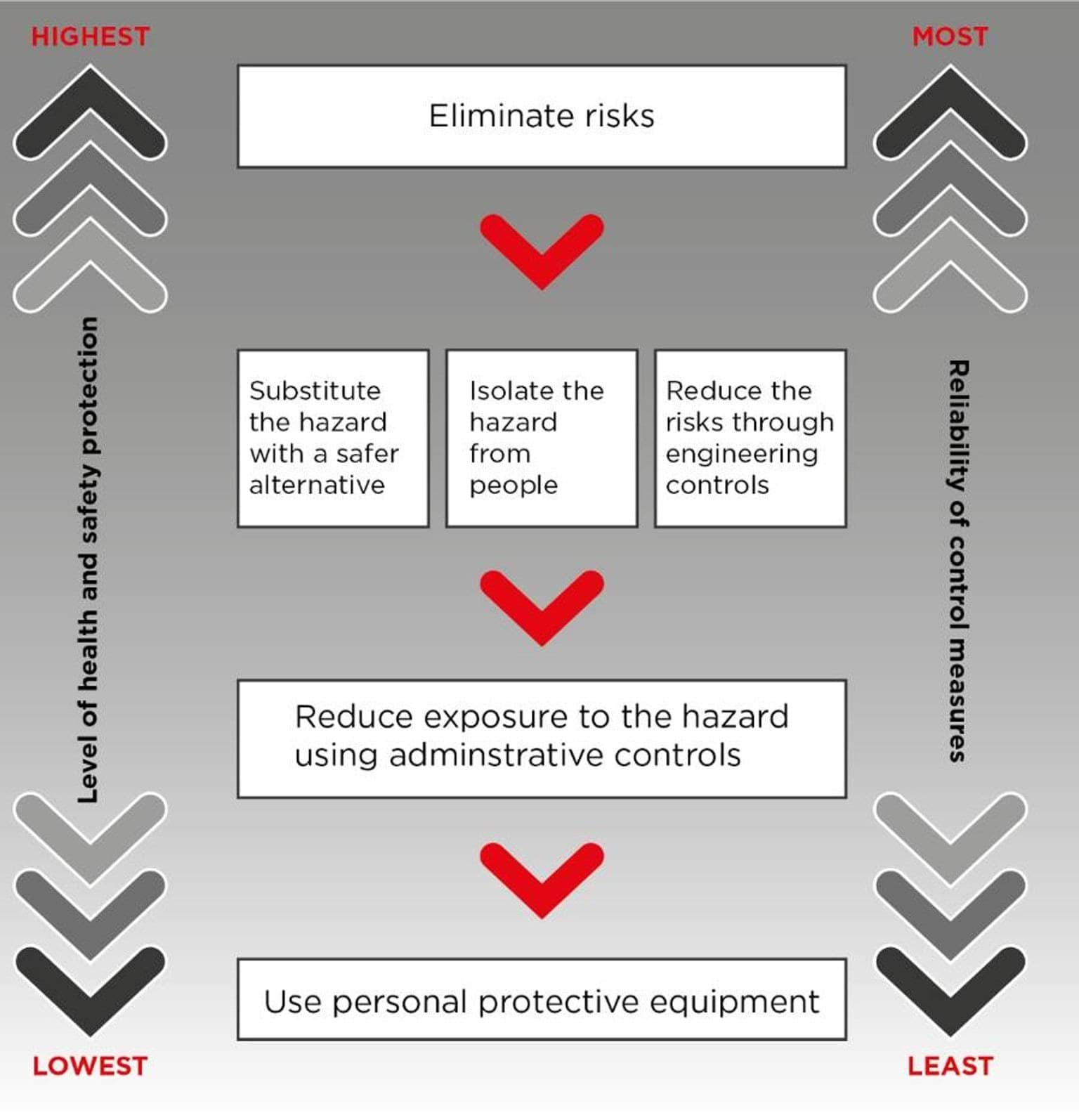
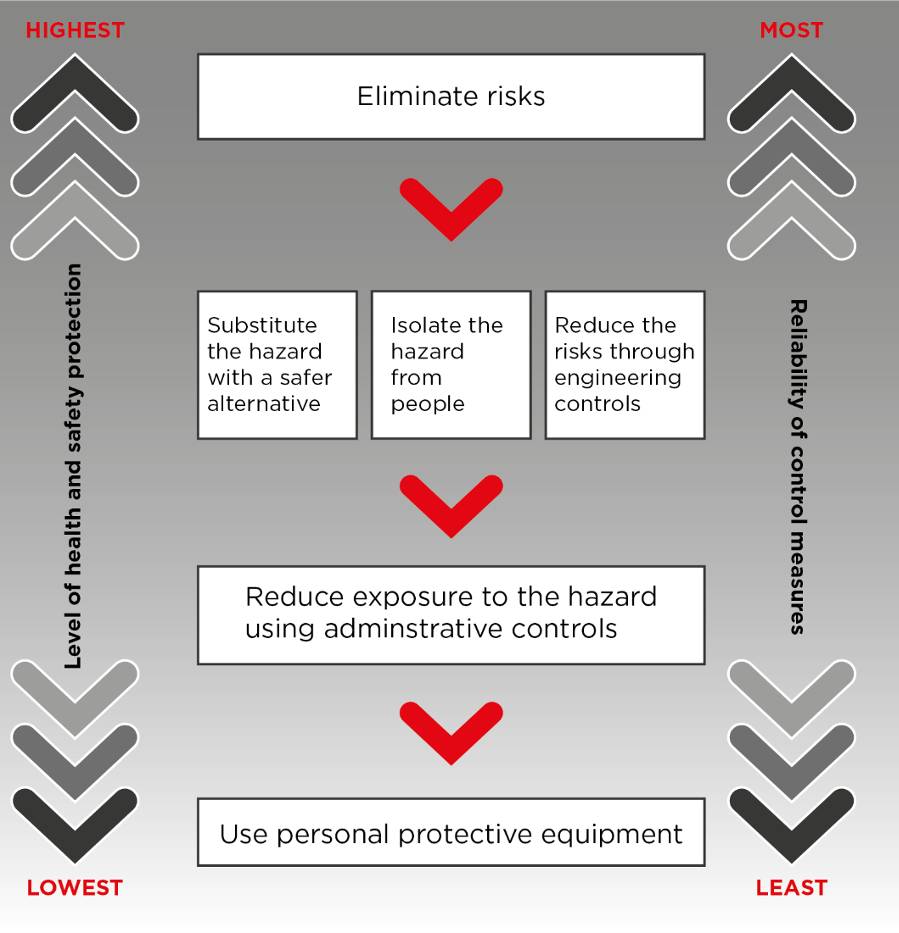
2.2. Hierarchy of controls
This is a model for managing occupational hazards in the workplace. The hierarchy ranks risk avoidance and risk mitigation strategies in decreasing order of reliability. Multiple control strategies are required to eliminate or minimise the risk of infection.
Hierarchy of controls
{kind=link}
2.3. Strategies to reduce COVID-19 transmission
COVID-19 infection prevention and control strategies should be aligned to the hierarchy of controls approach to risk.
Table 1. Hierarchy of controls and infection control strategies
| Hierarchy of controls | Example IPC strategies |
|---|---|
|
Elimination Removal of the virus from the workplace and therefore eliminate the risk of transmission. Elimination of the COVID-19 virus itself is unlikely.
|
Exclude unwell staff from the workplace Offer alternative work options for at-risk staff Screen staff and visitors prior to entry to the workplace Use telehealth to minimise face-to-face consultations |
|
Substitution Finding other ways to provide care that reduce potential for transmission. |
Use telehealth in place of face-to-face consultations. Consider conducting activities outdoors. |
|
Isolation Isolation of infected persons to prevent potential transmission. |
Use Class N negative pressure rooms for COVID-19 positive patients. If not available, use standard isolation rooms or single rooms with private bathrooms. Cohort groups. Use of patient zones. |
|
Engineering Changes to infrastructure or equipment or change systems of work. |
Optimise ventilation systems/zones in buildings. Use air cleaning devices. Consider the use of clear perspex screens (with caution). Vaccines. |
|
Administration Implementation of policies and protocols to guide practices that reduce risk. |
Implement policies such as:
|
|
Personal protective equipment Worn to protect the wearer from infection. |
Use transmission-based precautions. Use PPE (masks, respirators, gowns, gloves, and eye protection). |
Standard and transmission-based precautions
Guidelines for hand hygiene, respiratory etiquette, cleaning, waste management and linen management in clinical care of patients where COVID-19 is a potential or known risk.
3.1. Definitions
Standard precautions
Standard precautions are the minimum infection prevention and control practices that should be used with all patients in all settings where clinical care is provided, regardless of known or suspected infectious status. Standard precautions help prevent risk of exposure to COVID-19.
Standard precautions should be used regardless of whether the patient is suspected or confirmed to have any infectious disease (including COVID-19) when handling blood and body substances. Body substances include blood, secretions (including respiratory secretions) and excretions (excluding sweat), regardless of whether they contain visible blood; non-intact skin; and mucous membranes.
Standard precautions consist of hand hygiene, respiratory hygiene and cough etiquette, use of PPE, routine environmental cleaning, handling of linen, handling and disposal of waste and sharps, cleaning shared equipment, reprocessing reusable medical devices and aseptic technique.
Transmission-based precautions
Transmission-based precautions are implemented in addition to standard precautions when interacting with and caring for patients who have suspected or confirmed transmissible infections including COVID-19 infection.
For more information on standard and transmission-based precautions, see Australian Guidelines for the Prevention and Control of Infection in Healthcare (2019).
3.2. Hand hygiene
Hand hygiene is an important strategy in preventing transmission of many infections. Healthcare workers (HCWs) must perform hand hygiene in accordance with Australia’s national hand hygiene initiative.
Patients and visitors should also be educated about the benefits of hand hygiene and be offered the opportunity to clean their hands when appropriate.
Alcohol-based hand rub (ABHR) should be used unless hands are visibly soiled, in which case hands should be washed with liquid soap and water. In the healthcare setting, ABHR must contain 60%–80% v/v of alcohol and be registered with the Therapeutic Goods Administration (TGA).
All HCWs in direct contact with patients or a patient’s environment should be ‘bare below the elbows’ where possible:
- Bracelets, wrist watches and rings with stones or ridges should not be worn. A single flat ring or band may be worn but should not interfere with effective hand hygiene practice.
- Long sleeves should be avoided. If worn, sleeves should be rolled or pushed up above the elbow so as not to interfere with effective hand hygiene practice.
- Fingernails should be kept short and clean and nail polish should not be worn.
- Artificial nails (gel or acrylic) should not be worn.
- Cuts and abrasions should be covered with a waterproof film dressing.
3.3. Respiratory hygiene and cough etiquette
When coughing or sneezing, the mouth and nose should be covered with a disposable, single-use tissue. Used tissues should be discarded immediately into a bin. If a tissue is not available, then the cough or sneeze should be directed into the inner elbow. Hand hygiene must be performed after coughing, sneezing, using tissues, or after contact with respiratory secretions or objects contaminated by these secretions.
Physical distancing is recommended and should be maintained as much as practicable. In healthcare facilities, patients with symptoms of respiratory infections should sit as far away from others as possible and be provided with a surgical mask to wear. Facilities may place these patients in a separate area, if available, while waiting for care.
3.4 Environmental cleaning
Coronaviruses can persist on surfaces. While the risk of fomite transmission of COVID-19 is extremely low, it is still important to maintain a hygienic environment in healthcare and residential care settings by environmental cleaning.
Cleaning is the process of removing dirt and germs from surfaces. The most effective way to do this is by rubbing or scrubbing the surface with warm water and detergent, followed by rinsing and drying.
Routine cleaning
Regular routine cleaning of surfaces should be continued as a standard practice to prevent the build-up of grime, dust, mould, and bacteria. Cleaning without disinfection is sufficient for most settings.
Routine cleaning schedules, especially for frequently touched surfaces, should consider the building’s usage, the function of the organisation, and any industry-specific legislation or standards. It is highly recommended that routine cleaning be undertaken at least daily. Increasing the frequency of cleaning, for example to twice daily, may also be considered in areas that have a higher risk of COVID-19 contamination, such as in outbreak situations, and high traffic areas with frequently touched surfaces.
Examples
Cleaning schedules should state the surface to be cleaned, the product used, the cleaning process and who has responsibility for cleaning.
Routine cleaning schedules should follow the recommended frequencies listed in Australian Guidelines for the Prevention and Control of Infection in Healthcare.
Before cleaning, increase ventilation by opening doors and windows and using ventilation systems to increase fresh air circulation.
Methods for surface cleaning

{kind=link}
When dusting surfaces, use a damp cloth to stop dust particles from spreading into the air.
To clean soft furnishings such as lounges, carpets, rugs, and drapes, use a vacuum cleaner fitted with a high-efficiency particulate air (HEPA) filter, if available.
Frequently touched surfaces in outdoor areas, such as dining furniture, should be cleaned routinely with detergent and water.
Cleaners should wear PPE appropriate to the risk. In addition to respiratory protection this may include disposable gloves, apron, and safety eyewear to protect against chemical or blood and body fluid splashes.
Disinfection
For most surfaces, routine cleaning with detergent and water is sufficient to physically remove soil, contamination, and organic material. When there is contamination with infectious matter, cleaning with detergent and water should be followed by disinfection using an appropriate disinfectant.
Any disinfectant used must be a hospital-grade product with claims against coronavirus, selected from the Therapeutic Goods Administration (TGA)’s Australian Register of Therapeutic Goods (ARTG) list: Disinfectants for use against COVID-19 in the ARTG for legal supply in Australia | Therapeutic Goods Administration (TGA).
Disinfection methods:
- Two step method – the surface is first cleaned with detergent and water and then disinfected using an appropriate disinfectant.
- One step method – the surface is cleaned and disinfected using a two-in-one detergent and disinfectant product. This may be either a liquid solution or impregnated wipes.
Storage, cleaning, and disposal of equipment
Ensure cleaning and disinfecting products are used according to manufacturer’s instructions and are cleaned and stored safely and correctly. This includes keeping a register of chemicals and safety data sheets. Ensure these safety data sheets are readily accessible.
After cleaning and disinfection, place disposable cloths and PPE in a plastic rubbish bag and dispose of the bag in the general waste. Reusable cleaning cloths and mops should be machine washed at the warmest possible setting, using normal washing detergent. Avoid shaking out the items before placing them in the washing machine.
Cleaning and disinfection in areas with COVID-19 risk
Cleaning and disinfection should be implemented in spaces that have been used by a suspected or confirmed COVID-19 case. This includes isolation rooms and outbreak areas. Cleaning frequency should be increased, paying particular attention to frequently touched surfaces.
Terminal cleaning
When patients with COVID-19 are discharged or transferred, the rooms or zones they have used should undergo terminal cleaning.
Cleaners should wear PPE appropriate to the risk. This may include respiratory protection, disposable gloves, apron, and safety eyewear to protect against chemical or blood and body fluid splashes.
Before cleaning the room, remove the patient’s personal belongings. Consider removing any fabric privacy curtains and window curtains for laundering. For disposable curtains, follow local policy or follow manufacturer’s instructions, including checking the expiry date.
Cleaning after procedures
Following an aerosol generating procedure (AGP) on a COVID-19 patient, cleaners should wait 35-60 minutes before entering the room, depending on the air changes per hour within the room. For more information, see 'Aerosol generating procedures' under section 5.3 on Managing staff, visitors and outbreaks.
For procedure rooms (for example, CT scan, MRI) and consulting rooms with short patient stays (for example, ED, Urgent Care, fever clinics), frequently touched surfaces should be cleaned and disinfected between cases. The area should also be cleaned and disinfected as per local policies, for example, at the end of the session or day.
Shared equipment
To reduce the risk of transmission, equipment should preferably be disposable and either single-use or single-patient-use. If reusable equipment is used, it should be dedicated for the exclusive use of the patient until the end of their isolation period, if possible.
Reusable equipment that is shared must be cleaned and disinfected between each patient according to manufacturer's recommendations and using a suitable disinfectant. Equipment that cannot be cleaned and disinfected between patients should not be reused.
Electronic devices in isolation and outbreak areas
Mobile phones and other electronic devices such as tablets, laptops, touchscreens, remote controls, mouse, and keyboards can become contaminated. These electronic devices should not be taken into isolation rooms or outbreak zones unless necessary for clinical care.
If electronic devices are required, consider using a cover that can be wiped.
Devices should be cleaned and disinfected after use with each patient, following the manufacturer’s instructions. If manufacturer’s guidance is not available, consider the use of alcohol-based wipes containing at least 70% alcohol.
Note:
- Hand hygiene must be performed before and after using mobile phones and other electronic devices.
- Do not use or answer mobile phones when wearing PPE and avoid sharing mobile phones, headphones, or ear pods of any kind.
For more information, see How to clean your personal items used at work.
Alternative cleaning methods NOT covered in this guideline
Cleaning and disinfection methods such as ultrasonic waves, ultraviolet germicidal irradiation (UVGI), anti-microbial surface coatings and anti-viral blue light (aBL) continue to be developed. These technologies may not be sufficient for infection prevention and control in the context of COVID-19 and are not currently recommended as primary methods of disinfection.
New products and technologies must be registered by the Therapeutic Goods Administration (TGA) and should be implemented with due diligence. They should be used only as a supplement to the cleaning methods recommended above. They should not be used in lieu of good IPC practice.
Fogging and fumigation are not currently recommended as methods of disinfection.
3.5. Waste management
Health services should have an established waste management program for the collection and removal of general waste and clinical waste that complies with EPA (Environment Protection Authority Victoria) guidance and statutory regulations.
Waste generated in clinical settings should be segregated as per EPA advice IWRG612.1: Clinical and related waste – operational guidelines.
In most cases, COVID-19 waste can be disposed of as general waste. This includes used PPE generated in non-clinical care settings such as residential community care homes or general workplaces. In the context of COVID-19, PPE waste can be disposed of as general waste unless it is contaminated with blood or body fluids (this includes respiratory secretions).
Disposable components of equipment and other consumables are considered general waste unless they are contaminated with body fluids. For example, in healthcare settings, PCR and RAT swab sticks and containers are clinical waste, whereas the packaging and uncontaminated components are general waste.
Healthcare workers must refer to and always comply with their organisation’s policies and procedures.
3.6. Management of linen
Management of linen from a suspected or confirmed COVID-19 case should be in accordance with standard precautions and routine procedure.
Handle soiled laundry with minimum agitation (do not shake dirty laundry) to avoid contamination of the air, surfaces, and persons.
Linen that is heavily soiled with blood, body substances or other fluids (including water) should be contained in clear leak-proof bags.
Personal clothing that is usually laundered by the family should be placed in a plastic bag for transport.
Clothing, linen, mop heads and soft toys from health service settings should be laundered through a laundry service that is compliant with AS/NZS 4146:2000.
For residential settings, laundry should be washed at the hottest temperature the items can withstand. Use usual detergent and dry items completely.
Curtains and bed screens
Reusable and disposable curtains and bed screens should be changed if they are soiled or contaminated.
Consider replacing reusable curtains after transfer or discharge of suspected or confirmed COVID-19 cases.
Disposable curtains should be checked with the manufacturers for their efficacy against COVID-19; if unsure, dispose after transfer or discharge of suspected or confirmed COVID-19 cases.
Healthcare worker (HCW) uniforms
If at any time a HCW’s clothing becomes contaminated with blood or body fluid, the clothing should be removed as soon as practical and before the HCW attends to other patients. If skin is contaminated with blood or body fluid, the HCW must remove contaminated clothing or PPE, wash any affected skin (if skin is broken refer to organisation policy on blood exposure), then perform hand hygiene.
Recommendations for managing uniforms and clothing:
- have dedicated work clothes (such as scrubs or a uniform)
- change out of work clothes at the end of the shift before leaving the building
- perform hand hygiene after handling dirty items of clothing
- launder uniforms after each wear using the hottest temperature that the items can withstand. Use usual detergent and dry items completely.
3.7. Signage
Appropriate signage about infection prevention measures should be displayed in clinical areas and in non-clinical areas such as lifts, administrative areas, cafeterias, waiting areas, facility, and ward entry points.
At the entry to patient care areas with COVID-19 risk, signage should indicate that transmission-based precautions and PPE are required.
In clinical and non-clinical areas, signage about physical distancing should be widely displayed.
3.8. Occupational exposure to COVID-19
The occupational exposure risk for COVID-19 is via inhalation of or splash to eyes, nose, or mouth with respiratory particles. Where such an exposure occurs, notify the immediate supervisor or manager for management via organisational processes and carry out first aid immediately:
- eyes—rinse thoroughly while eyes are open with water/normal saline
- mouth—spit out and rinse with water several times.
Caring for a patient whilst wearing the correct PPE is not considered an occupational exposure in this context.
Personal protective equipment (PPE)
Guidelines for healthcare workers on using PPE in healthcare and community settings where COVID-19 is a potential or known risk.
4.1. Recommended PPE
PPE is a critical part of infection prevention and control. PPE is a strategy within the hierarchy of controls strategy and is considered one of the least effective controls, it is therefore seen as the last line of defense.
The following guidance identifies the minimum level of PPE recommended for the protection of healthcare workers in the context of COVID-19. Additional PPE may be used, as determined by local risk assessment, organisational policy, or worker preference.
Hand hygiene must never be compromised when using PPE. In healthcare settings, the 5 moments of hand hygiene should be followed.
Staff utilisation of PPE in non-patient areas
Organisational guidelines on the use of facial protection should be consistent with current jurisdictional guidance, which may include government directions, Victorian Department of Health or Commonwealth Department of Health and Aged Care guidance.
The following respirators and face masks may be appropriate, based on local policy and other relevant guidance. They are listed in order of higher to lower levels of protection:
- N95 or P2 respirator mask: These are high filtering masks. If they fit correctly, they provide the best protection. Respirator masks with straps that go around the head are likely to fit better and give more protection than respirator masks with ear loops.
- KN95 mask or KF94 mask: These are high filtering masks but are not as well fitted as a respirator. They usually have ear loops, so they do not achieve as good a seal between the mask and the face as an N95 or P2 respirator mask.
- Surgical or medical masks: These provide protection when worn correctly, fitting snugly over the nose, mouth, and chin.
Health services should employ risk assessment in determining mask requirements in public-facing areas (for example, visitor's enquiry desk). Health services may consider not employing mask requirements during periods of low community COVID-19 transmission risk.
In periods of high community COVID-19 transmission risk (informed by local epidemiology, COVID-19 hospitalisation numbers or in areas with high levels of immunocompromised patients), health services should require staff to wear masks with the choice of surgical mask or P2/N95 respirator at the individuals or services discretion and according to their fit test profile.
Individual staff choice to wear a mask should be maintained in non-patient facing areas, for example, corporate support offices. Surgical masks and P2/N95 respirators should be made available to all staff at all times to support choice and risk (for example, cases returning to, or contacts attending, the workplace).
Staff utilisation of PPE for clinical and patient-facing areas
P2/N95 respirators are recommended to be worn by all staff in all patient facing areas (including nurses’ stations or administration areas in wards) when COVID-19 transmission risk is high and an optional choice of surgical mask or P2/N95 respirator when COVID-19 transmission risk is low. At a minimum, surgical masks are recommended in clinical and patient-facing areas with N95/P2 masks to be used:
- for COVID-19 cases returning to work
- for close contacts attending the workplace
- according to the preference of the individual staff member, or
- as directed by the health service.
Health services are supported to recommend P2/N95 respirators for specific groups in high-risk areas as determined by the health service.
Health services should ensure that (subject to availability) P2/N95 respirators are available for staff based on their preference and fit test/fit check profile.
PPE when caring for patients with confirmed or suspected COVID-19 infection
The following transmission-based precautions are recommended for the care of COVID-19 patients. COVID-19 patients include suspected, probable, and confirmed cases, and contacts and patients who are recommended to isolate or quarantine.
Patients should always wear masks when outside of the isolation room (for example, during transfers, procedures, or diagnostics), noting that P2/N95 respirators offer a higher level of source protection and should be worn where it's safe to do so.
Table 2: Transmission-based precautions for COVID-19 – recommended PPE
| P2/N95 respirator* | Eye protection | Disposable or reusable gown/apron | Disposable gloves |
|---|---|---|---|
| Yes | Yes | Standard precautions** | Standard precautions |
* P2/N95 respirators should be fit tested.
**Standard precautions:
- Wear gown and gloves when a risk assessment indicates potential exposure to blood or body fluids, including respiratory secretions (for example, in symptomatic patients, or in aerosol generating behaviours or procedures). This applies to all settings, in all circumstances.
- Long-sleeved gowns may offer higher level protection.
- Hand hygiene should not be compromised by PPE use.
Single-use PPE
PPE that is labelled and marketed as single use should not be reused. The only exception is during periods of critical short supply when health services should implement clear guidance regarding re-use.
Reusable PPE
PPE that is labelled and marketed as reusable may be reused following cleaning and disinfection between each use. Reusable PPE should be inspected before each use to confirm that it is undamaged and still fit for purpose.
PPE for visitors
Masks are recommended to be worn by visitors to clinical areas at all times. Health services may consider requiring P2/N95 respirators to be worn by visitors to high-risk areas and during periods of increased transmission risk.
4.2. Donning and doffing PPE
PPE should be donned (put on) and doffed (taken off) in a controlled and safe environment to reduce the risk of contamination to self, others, or the surrounding environment. While doffing PPE it is particularly important to prevent contact between contaminated PPE and clean surfaces, skin, or clothing.
Staff should be trained and competent in donning and doffing (including one step or 2 step removal methods) and performing a fit check(see 4.3. Respiratory protection) when a P2/N95 respirator is donned. Staff not familiar with PPE may need the help of a PPE spotter or buddy to monitor and support safe practice. Mirrors may also be used to ensure that PPE has been donned correctly.
Table 3: Standard sequence for donning and doffing PPE
|
Donning (putting on) |
Doffing (taking off) |
|---|---|
|
Prior to entering a room or zone, perform hand hygiene and don:
|
On leaving the room or zone, doff:
|
* A fit check must be completed when donning a respirator
** Gloves and gown may be removed together in a one-step method or as two separate steps.
For more information, see the following resources:
Donning and doffing stations
Positioning donning and doffing stations:
- Station should be located in places that are protected from excess foot traffic, contaminated environments, and from potential handling by patients, residents, or others.
- Stations must have sufficient room for staff to comfortably and safely don or doff without risk of contamination to or from themselves and the environment.
- Whenever possible maintain a minimum 1.5 metre distance between donning and doffing stations.
- If the doffing station is inside the patient’s room, where possible maintain a minimum 1.5 metre distance from the patient.
- The doffing station should be located immediately outside or inside the patients’ room or the designated isolation area/zone, as close as possible to the door.
Stocking PPE stations:
- Ensure stations are cleaned and restocked on a regular schedule.
- A sufficient volume and range of recommended PPE must be available for staff.
- Avoid stacking excessive volumes of PPE on tables or floors at donning stations: PPE must be stored clean, dry, and protected from environmental contamination.
- Waste bins (including a clinical waste bin) should be available at doffing stations.
- Display signs to identify the station. Display PPE sequence posters.
- Unused PPE that has been stored inside an isolation room is considered contaminated and must be discarded once the patient is cleared and the stock is no longer required.
PPE spotters
The use of a PPE spotter program is optional and may not be required or appropriate in all situations.
The purpose of a PPE spotter is to support safe and effective donning, doffing and use of PPE, particularly by staff who are less familiar with wearing PPE.
PPE spotters should be easily identifiable and assigned to observe the real time PPE donning and doffing process by staff, contractors, and visitors to identify and correct any deficits or breaches in PPE selection and use.
PPE spotters should be trained to explain, promote, and model safe and effective use of PPE.
The PPE spotter’s functions may include:
- Educating others to identify which PPE should be worn, where and when it should be worn, and when it should be changed. This includes donning and doffing sequences.
- Observing and assisting when others are donning or doffing PPE. The spotter should give calm and clear directions by calling out each step of the sequence. They should proceed at a controlled and careful pace, confirming correct completion of each step before moving to the next step.
- Monitoring PPE use and giving on-the-spot feedback to assist and correct any breaches or unsafe practices. This should be done in a positive way that promotes behaviour change and offers collegial support.
- Conducting compliance audits to monitor and report staff practice. The spotter should have a pathway to escalate unresolved concerns, deficits, and ongoing practice breaches.
Additional responsibilities may include assisting with the investigation and follow-up of staff experiencing adverse effects of PPE use (for example skin or pressure injuries).
PPE breaches
Facilities should establish workplace protocols to investigate and manage PPE breaches.
If there is a breach in PPE or potential self-contamination, staff should notify the direct supervisor and follow organisational procedures for incident reporting.
4.3. Respiratory protection
Masks and respiratory protection
Individual tolerances, fit test results, and preferences must be considered when choosing the appropriate respiratory protection equipment (RPE).
Cloth face masks are not recommended for staff working in healthcare, residential aged care, or supported accommodation settings. Cloth face masks may only be worn by HCWs when arriving or leaving the facility.
Surgical masks and P2/N95 respirators can be worn continuously for up to 4 hours. A mask should be disposed of after 4 hours, or earlier if it becomes damp or soiled, hard to breathe through, loses its shape and no longer conforms to the face, or before going on a break.
Before P2/N95 respirators are used, each user should undergo fit-testing to verify which brands of respirator will seal to their face. The user should also perform a fit check each time the respirator is donned to confirm that it seals.
To find out more, see Face mask do's and don'ts.
Fit testing
Fit testing is the process of verifying which brand, model and size of respirator will seal to the face of an individual. Fit testing is carried out using specialised equipment. Fit testing can be conducted by individual health organisations or independent contractors using either qualitative or quantitative methods. Both methods are valid and appropriate.
All employees who wear a respirator should undergo fit testing to ensure that an effective face seal is achieved and to comply with the Australian and New Zealand Standard AS/NZS 1715:2009.
For staff unable to pass a fit test, an alternative respirator (such as a PAPR) should be made available. There must be alternatives available for staff required to wear P2/N95 respirators unable to pass a fit test.
Students on placement who are required to wear a P2/N95 respirator should be fit-tested, either prior to commencement, as part of their onboarding process.
If fit testing has not yet been carried out, a P2/N95 respirator should still be used in preference to a surgical mask. A respirator, whether fit-tested or not, must always be fit-checked (see below) every time it is donned.
Staff should wear their PPE eye protection and facial dressings (if being used) while fit testing to ensure the protection does not interfere with the respirator fit or facial seal.
Fit checking
Fit checking is the process of evaluating the seal of a P2/N95 respirator at the point of use. Staff must perform a fit check every time they put on a P2/N95 respirator to confirm that a seal is achieved. A fit check is a distinctly different function to a fit test (above).
The procedure for donning and fit checking a respirator:
- Place the respirator on the face so the top rests on your nose and the bottom is secured under your chin.
- Place the top strap or tie over the head. Position it high on the back of the head.
- Pull the bottom strap over your head. Position it around your neck and below your ears.
- Place fingertips from both hands at the top of the nosepiece. Using two hands, mould the nose area to the shape of your nose by pushing inward while moving your fingertips down both sides of the nosepiece
- Ensure the head straps and respirator edges around the facial seal are not twisted, wrinkled, or folded.
- Check that the respirator has a negative pressure seal by covering the respirator with both hands and inhaling sharply. If the respirator is not drawn in towards the face, or if air leaks around the face seal, readjust the respirator.
Always refer to the manufacturer’s instructions for fit checking each brand or type of P2/N95 respirator.
Selection of respirators
Respirators used for HCW protection must be registered with the Therapeutic Goods Administration (TGA) as medical devices for use in health care, surgery, clinical or medical settings. This can be confirmed by checking the TGA Australian Register of Therapeutic Goods (ARTG) listing. TGA registered devices have a 6-digit Australian Register of Therapeutic Goods (ARTG) reference number and a GMDN code which identifies if it is registered for HCW use or use by the public. See 'TGA listed respirators' in References under section 8.3.
Respirators with exhalation valves
Exhalation valves allow infectious particles to be exhaled from an infected person into the environment. Respirators with exhalation valves are not appropriate for use in health services as they do not provide source control and so are not fit for purpose where the required protection is bidirectional.
Elastomeric respirators
Elastomeric respirators approved by the TGA may be considered an alternative form of respiratory protective equipment. A risk assessment should be performed by the facility. Elastomeric respirator use must be accompanied by training programs for safe use, decontamination, and maintenance. In addition, the wearer should be fit-tested and receive training in safe use, donning and doffing, and infection prevention and control.
Elastomeric respirators with exhalation valves that do not filter exhaled air are not appropriate for use. They do not provide source control and so are not fit for purpose where the required protection is bidirectional.
Powered air-purifying respirators (PAPR)
Powered air purifying respirators (PAPR) use a blower to force air through a filter into the breathing zone of the wearer. A PAPR may have a tight-fitting half or full facepiece or a loose-fitting facepiece, hood, or helmet.
PAPRs meeting the requirements of AS/NZS 1715: Selection, use and maintenance of respiratory protective equipment (or its equivalent, such as an equivalent US or European Standard on respirators) may be considered as an alternative form of respiratory protective equipment in some circumstances, including:
- for increased comfort during prolonged RPE use (such as an entire shift)
- Where staff are routinely performing intubation in COVID-19 intensive care unit (ICU) areas
- when staff are unable to achieve a face seal; for example, due to beards, facial contours, deformity, allergy, or injury; for example, pressure ulcers from P2/N95 masks.
PAPRs provide additional comfort and visibility when healthcare workers must stay in the patient’s room continuously for prolonged periods.
In addition to protecting the wearer from external pathogens, PAPR that have filters for expired air also function as source control if the wearer is infectious.
PAPRs are available in distinct types, weights, and comfort levels. When selecting a PAPR, avoid models that do not filter the exhaled air. Consider face and skin protection. Partial-face PAPRs have advantages for verbal and visual communication but leave the eyes and other skin surfaces exposed to the risk of splash or spray contamination.
External surfaces of the PAPR should be considered contaminated, particularly the filter, which is a concentration point for particles. Care should be taken when doffing to avoid transferring contamination from the PAPR to self or clothing.
Reusable PAPR components must be cleaned and disinfected after use as directed in manufacturer's instructions and stored to prevent contamination. Documented cleaning and disinfection instructions should include cleaning methods, detergent agent, and disinfection agent (using TGA-listed products with claims for effectiveness against COVID-19), frequency and responsibility for cleaning.
Considerations for implementation:
- PAPR may not provide any additional protection compared to a well-sealed P2/N95 respirator.
- Some models of PAPR rely on a facial skin seal. These will require fit testing.
- Employers must ensure that appropriate cleaning, storage and charging facilities are available.
- PAPR should only be used by healthcare workers trained and competent in safe donning and doffing sequences, decontamination / cleaning after each use, when and how to change filters and charging of the battery, etc.
- PAPR should be used according to the manufacturer’s instructions, including recommended use, filter position, reprocessing of re-usable components, and battery use.
- PAPR selected for use during aseptic procedures should not pose a risk to the aseptic field.
- Employers need to allow for additional time for employees to don/doff and undertake tasks such as maintenance and decontamination (compared to the use of disposable respirators).
- Some employees may not be able to wear a hooded PAPR and this should be considered for each employee.
Respiratory protection programs (RPP)
Respiratory protection programs implement strategies designed to protect workers from workplace respiratory hazards, including COVID-19. All Victorian health services where health care workers, including volunteers and students on clinical placement, have the potential to be exposed to respiratory hazards are required to establish and maintain an RPP. See Victorian Respiratory Protection Program.
Employers are responsible for:
- completing a risk assessment that identifies staff who require P2/N95 respirators
- ensuring users of respirators undergo AS/NZS 1715:2009 approved fit-testing. Either qualitative or quantitative methods are valid and appropriate
- providing education and training on the safe and appropriate use of selected PPE.
Employees are responsible for:
- using PPE as instructed by the employer
- reporting any damage, defects, or malfunctioning PPE
- reporting any physical or medical limitations that may impact their ability to safely wear PPE.
Masks for use by patients
In clinical areas, communal waiting areas, public access areas, and during transportation, it is recommended that patients suspected or confirmed to have COVID-19 wear a face mask, noting that respirators provide higher level protection than surgical masks. Due to this, respirators should be worn when safe to do so.
A face mask is not recommended when a patient’s breathing or clinical care may be compromised.
It is recommended that children two years old and under never wear a face covering or mask due to choking and strangulation risks.
Other patients should be provided with either a surgical mask or P2/N95 respirator according to their preference.
4.4. Protective eyewear
The eyes, mouth, and nose all contain mucosal surfaces that are potential routes of acquisition of COVID-19. Eye protection has been associated with a lower risk of infection and provides a physical barrier to the deposition of virus-containing particles.
Protective eyewear should be used (in addition to other required PPE) by healthcare workers providing direct care or working within the patient zone with individuals with confirmed or suspected COVID-19.
Eye protection options include face shields, goggles, and safety glasses (including single use and reusable models) but does not include regular prescription glasses.
When wearing a P2/N95 respirator, it is important to select compatible eye protection that can be correctly positioned and does not interfere with or breach the respirator fit or facial seal. Staff should have eye protection available at the time of fit testing.
Goggles and safety glasses
Closely fitted wrap-around goggles or safety glasses that meet Australian Standards AS/NZS 1337.1-2010 (personal eye protection) provide reliable eye protection from splashes, sprays, and respiratory droplets that can come from multiple angles. Standard prescription glasses, contact lenses or safety glasses that are not wrap-around do not provide adequate protection and are not recommended as eye protection.
For optimal protection, goggles must fit snugly, particularly from the corners of the eye across the brow. Other types of protective eyewear include safety glasses with side-shield protection.
Face shields
Single-use or reusable face shields are an alternative to goggles or safety glasses. Face shields are particularly useful for splashes and sprays of blood or body fluids, depending on the type of work performed.
All face shields should provide a clear plastic barrier that covers the face. They should extend below the chin and to the ears, and there should be no exposed gap between the forehead and the shield’s headpiece. Face shields which have a gap between the forehead and the headpiece are unsuitable for use in the operating theatre, birthing suite, or when aerosol-generating procedures are performed on COVID-19 cases, unless additional eye protection is worn under the face shield. These shields are, however, an appropriate form of eye protection in non-high-risk areas.
Wearers of prescription glasses can wear a face shield or one of various brands of goggles which may be worn over prescription glasses, or alternatively, safety glasses with prescription lenses.
Comparing different types of eye protection
Fitted wrap-around goggles/safety glasses have these advantages:
- flexible frames easily fit facial contours
- good eye protection is provided by enclosing the eyes
- prescription safety lens may be fitted.
and these disadvantages:
- prolonged wear may increase the risk of skin injuries, particularly if the seal is tight
- they do not cover other areas of face or mask/respirator
- they do not deter the wearer from touching the front of their face, mask, or respirator
- they may not be able to be worn over prescription glasses
- reusable safety glasses require cleaning and disinfection after use
- lenses may degrade or become scratched over time
- higher risk of fogging
- reflections on the shield can impede vision.
Face shields have these advantages:
- can be worn over prescription glasses
- adjustable head band attaches firmly and fits snugly against the forehead
- provide additional protection of face and mask/respirator from contamination (blood or body fluid splash, spray, droplet, cough, or sneeze)
- the wearer’s eyes are more visible, which may be important when caring for some patients
- less risk of fogging
- the wearer is less likely to touch their face or mask.
and these disadvantages:
- gaps to the sides and underneath may allow virus-contaminated droplets to reach mucous membranes.
Note: Face shields do not filter air and are not an alternative to wearing a mask or respirator.
How to remove protective eyewear
When doffing eye protection, the wearer should avoid touching their face near their eyes. Hold glasses by the arms and goggles and face shields by the headband at the back of the neck.
How to clean and disinfect protective eyewear
Protective eyewear labelled as ‘single use’ should be discarded after use and not reused.
Reusable protective eyewear should ideally be issued for individual person use. It must be cleaned and disinfected before and after use or reuse. Manufacturers’ instructions should be followed.
Eyewear can be cleaned and disinfected individually at the point of use or returned to a central point for batch cleaning of multiple units of eyewear.
For more information, see How to safely clean your reusable face shield.
4.5. Gowns
Gowns protect clothing and skin against blood and body fluids; long-sleeved gowns offer the highest level of protection.
The type and level of gown should be selected according to a risk assessment of clinical requirements (for example, sterile versus non-sterile) and blood or body fluid (including respiratory secretions) exposure risk such as spray, splash, or high volume.
Disposable gowns that are visibly soiled or wet should be taken off and discarded. Reusable gowns that are visibly soiled or wet should be taken off and laundered in compliance with Australian Standards AS/NZS 4146:2000 (Laundry practice).
4.6. Gloves
Gloves provide protection and may be used in standard and contact precautions.
General principles:
- Gloves used in healthcare, residential aged care and supported accommodation settings must be of medical grade in compliance with Australian Standards AS/NZS 4011 and ISO 11193 (Single-use medical examination gloves). Vinyl gloves are not recommended for clinical care.
- Gloves must not be washed or have alcohol-based hand rub applied as this may damage the glove’s integrity.
- Double gloving is not recommended.
Extended use of PPE does not apply to gloves. Gloves are never a substitute for hand hygiene and MUST always be changed between patients and hand hygiene performed. The 5 moments for hand hygiene must always be followed.
Gloves must be changed:
- after procedures
- when contaminated with blood or body fluids or other substances
- between patients.
4.7. Extended use of PPE
Extended use of PPE refers to wearing the same PPE for repeated close episodes with more than one patient, without removing them between each patient. Extended use of PPE is only permitted when caring for a cohort of patients with the same confirmed infectious condition and if the patient does not have another infectious condition.
In these situations, extended use of PPE can be less of a risk than frequent donning and doffing.
A surgical mask or P2/N95 respirator can be worn continuously for up to four hours. A mask should be disposed of after four hours or earlier if it becomes damp or contaminated, hard to breathe through, loses its shape and no longer conforms to the face or before going on a break.
Gowns do not need to be removed between patients unless they are visibly soiled or high risk/close contact tasks are being performed.
Extended use of PPE does not apply to gloves.
All PPE is required to be changed when leaving the COVID-19 clinical area or moving between COVID-19 clinical areas and non-COVID-19 areas.
Preventing PPE-related facial injuries
Prolonged use of tight-fitting facial protection, including respirators, face shields and goggles can contribute to skin injury. This is due to pressure and shear forces, friction, and the accumulation of moisture under the respirator. Skin that is excessively moistened by sweat and humidity is susceptible to irritation. Dry skin may become inflamed by cracks and fissures. Skin conditions such as rosacea, dermatitis, atopic eczema, dry/chapped lips, and acne can be exacerbated by the heat and sweating which occurs when wearing PPE.
Employers and employees should work together to minimise the risk of facial skin injury related to respirator use.
Employers should:
- support workers who wear respirators to monitor for skin injury
- act when workers report discomfort or skin injuries
- provide fit testing for every worker who wears a respirator
- provide sufficient supplies of a fitted respirator for each worker
- provide appropriate training for workers in performing fit checking, using respirators, and preventing facial injuries when wearing respirators.
Staff should:
- report discomfort or skin injury arising from their respirator to their supervisor
- seek a medical assessment and referral to a dermatologist if an allergic reaction to PPE occurs
- if a dressing is placed between the skin and respirator, ensure it does not interfere with the function of the respirator. The dressing should be worn during fit testing to confirm an effective seal.
The best prevention for respirator-related skin injury is to limit use to those times when a respirator is required for protection such as when working with identified COVID-19 risk.
Wherever possible, remove mask every 2 to 4 hours for up to 15 minutes and align with break times.
Maintain good skin care practices:
- Keep the skin clean and hydrated by drinking plenty of fluids.
- Avoid alkaline soaps/cleanser/toner and irritant chemical solutions.
- Keep facial skin care regime simple and avoid wearing makeup when wearing respirators.
- Moisturise using pH balanced products, use lip balm and avoid fragranced products.
- Apply liquid skin sealant/protectant, moisturising lotion, or barrier creams on skin surfaces that will be in contact with PPE. This may help prevent friction injuries without interfering with the fit of respirators or eye protection. Apply at least 30 minutes before wearing PPE. Allow to fully dry before applying PPE.
Using hydrocolloid or foam facial dressings
A thin hydrocolloid or foam dressing may be placed on facial pressure areas caused by PPE. Ensure dressings are wrinkle-free so that the respirator seal is not impaired. Some adhesives may be irritating for some people—cease use and seek treatment if symptoms of contact dermatitis occur.
Dressings may reduce the fit of respirators. Fit testing should be repeated with any dressings in place. Certain respirators are compatible with certain types of dressings. For more information, see Prevention and management of skin injury from PPE.
Staff who develop a pressure injury may need to be trialled with a different type of respirator or eye protection or may need to be re-deployed to a different area which does not necessitate prolonged use of respirators.
Where there is difficulty managing a pressure-related skin injury or achieving an adequate fit, further options will need to be discussed with management, an infection prevention and control consultant, or an occupational health medical practitioner, general practitioner, or dermatologist.
For more information, see Caring for your skin when wearing PPE.
4.8. Controlling heat stress while wearing PPE
PPE can reduce the body’s ability to cool off by evaporating sweat. Wearing PPE in hot weather, usually outdoors, may lead to heat stress. The effects of PPE-related heat stress may range from discomfort through to a life-threatening condition such as heat stroke.
The individual and the employer should minimise the risk of developing a heat-related illness.
Some key risk factors for developing a heat-related illness are:
- air temperature, wind and air movement, and radiant heat (from the sun or other sources)
- workload and task complexity
- period of exposure, long shift
- availability of a cool rest area and drinking water
- physical fitness of the worker (including acclimatisation and any pre-existing conditions)
- clothing (including the use of respiratory protection)
- the individual’s understanding of heat strain risk.
Strategies for managing common risks related to wearing PPE in the heat:
- Use a PPE spotter or buddy system.
- Regularly check surgical masks or respirators for moisture due to sweating and for signs of pressure injuries.
- Select the lightest level of gown for the required protection as determined by the risk of splash or spray.
- Wear a single layer of lightweight/cool clothing under PPE.
Managing staff, visitors and outbreaks
Guidelines for preventing and controlling outbreaks of COVID-19 in healthcare settings, including managing workers, cohorting and zoning patients and residents.
5.1. Workforce strategies
Workers in sensitive settings
People working in sensitive settings where there are many people vulnerable to the severe effects of COVID-19 should monitor their personal health. These settings include:
- residential care facilities (including aged care, disability, and other services)
- other care facilities
- healthcare premises (including when health care services are provided in people’s homes).
Workers in sensitive settings should not present for work when unwell with symptoms of an acute respiratory infection. This is defined as the recent onset of new or worsening acute respiratory symptoms as follows:
- cough
- breathing difficulty
- sore throat
- runny nose/nasal congestion with or without other symptoms.
Workers who are confirmed cases
Health services should have a requirement that workers who are confirmed COVID-19 cases do not attend the workplace for a minimum of 5 days (return on day 6) following the onset of symptoms (or date of the first positive test if asymptomatic) and until the resolution of acute symptoms.
On the worker's return, on day 6 and until 10 days following the onset of symptoms (or date of first positive test if asymptomatic), additional mitigations should be required by health services. This includes the worker being required to use a P2/N95 respirator and have separate breakout areas, where possible. Additional RAT testing may also be considered to support decision-making regarding a worker returning to work.
Health services can consider allowing an earlier return to work in circumstances where a worker's attendance at work is required to prevent a significant risk to safe service delivery. In these situations, a local risk assessment should be undertaken, and additional mitigations should be in place including the worker:
- wears a P2/N95 respirator
- is asymptomatic (or all acute symptoms having resolved)
- returns a negative COVID-19 RAT
- uses separate breakout areas.
Staff must never be compelled to return to work when unwell.
Workers who are close contacts
Routine isolation of workers (or patients) who are close contacts is not required. This includes workers providing in-home care to people at high risk of COVID-19.
Health services should make it a requirement for close contacts to wear a P2/N95 respirator for 7 days after the exposure (or date of diagnosis of the first case within the household if cohabitating with the first case).
Workers who are close contacts should undertake rapid antigen testing (RAT) 24 hours apart, for 5 days out of 7 days, after being identified as a close contact and test when symptomatic.
Routine asymptomatic testing of staff is not supported when COVID-19 transmission risk is low. It is recommended that individual health services consider implementing staff surveillance testing in specific circumstances, such as during an outbreak.
Healthcare worker vaccination
Health facilities should implement a COVID-19 staff vaccination program that is in line with current Department of Health guidance, see Vaccination for healthcare workers. Workers in sensitive settings are particularly recommended to keep their vaccination status up to date.
Work options for higher-risk workers
Service providers should identify any healthcare workers in the higher risk population, including pregnant workers. Managers should consider offering these workers duties in settings with reduced risk of exposure to patients with confirmed or suspected COVID-19. In all cases, refer to health service guidelines and apply clinical judgement when determining work restrictions. Seek advice from the organisation’s occupational health and safety team.
Consider these work options:
- Redirect the worker to care for patients who are not confirmed or suspected to have COVID-19.
- Redirect into non-clinical or clinical roles that do not have contact with patients who have confirmed or suspected COVID-19.
- Arrange alternatives such as working from home, teleconferencing or videoconferencing.
- Ensure shared offices and other spaces occupied by this group meet any density and physical distancing requirements and consider department advice relating to ventilation.
Staff education and training
Staff should be trained in basic infection prevention and control practices and procedures relevant to their roles and settings, including:
- standard precautions and transmission-based precautions
- hand hygiene
- environmental hygiene
- waste and linen management
- outbreak management
- safe and appropriate use of PPE.
For further information on educational opportunities, see 'COVID-19 and IPC education' in References under section 8.4.
Safe staff amenities
Health services staff must have access to safe facilities to take meal breaks, use bathrooms, and access training and other necessary activities without compromising physical distancing and infection prevention control measures.
In situations where staff are permitted to return early from isolation, they should not take breaks with other staff.
Food services staff
Any staff appropriately trained to use the required PPE may enter a COVID-19 patient care area, including food services staff. However, non-essential staff should be restricted from entering COVID-19 patient care areas where possible.
Local facility processes will detail how meals and beverages are delivered to patients in COVID-19 patient care areas, based on PPE availability, staff training and workflow considerations.
Unused food items should be discarded.
Disposable crockery and cutlery are not necessary. Standard precautions should always be used when handling used crockery and cutlery. Crockery and cutlery can be washed using a domestic dishwasher (on the highest temperature) or a commercial dishwasher on the 75°C setting. If a dishwasher is not available, wash with hot water and detergent, rinse and leave to dry.
Food trolleys that have been used in any COVID-19 clinical areas should be cleaned and disinfected before reuse.
5.2. Isolation, cohorting, zoning and patient movement
Isolation
Risk-based assessments should be undertaken to determine the appropriate location for patient care. Where the safest option is not available or appropriate, a risk-based decision should be made by the senior admitting staff in consultation with service leaders and local infection prevention and control (IPC) teams (if available).
The priority room allocation for isolation of confirmed or suspected COVID-19 patients should consider the following, according to facility resources:
- Isolation in Class N negative pressure rooms with ensuite facilities, with or without a dedicated anteroom, is the first choice where available.
- Isolation in single rooms with ensuite facilities and without negative pressure airflow, but with augmented ventilation (such as a portable air cleaner).
- Isolation in single rooms without both ensuite facilities and negative pressure airflow, but with augmented ventilation (such as a portable air cleaner).
- Cohorting in dedicated COVID-19 wards or wings physically separated from other patient areas.
Co-location of COVID-19 and non-COVID-19 patients in shared spaces should only be used as a last resort where there are complex circumstances. This must only be implemented after careful risk assessment and consideration of system capacity through consultation with IPC staff, Occupational Health and Safety, and service leadership (for example, executive staff responsible for operations).
When co-location of COVID-19 and non-COVID-19 patients is implemented, services should maximise the use of mitigations such as personal ventilation hoods, PPE and portable air cleaners where possible.
Note: If ensuite facilities are not available, a dedicated toilet or commode should be allocated. Bathroom exhaust fans should always be turned on. Avoid the use of rooms that are positively pressurised with respect to corridors.
Cohorting
Cohorting is described as grouping individuals with the same condition or same laboratory-confirmed infection in the same location (a room, ward section or building).
During periods with high prevalence and or during local outbreaks, facilities may consider implementing cohort isolation in a designated COVID-19 care zone.
The goal of cohorting patients and the staff that attend to them is to minimise opportunities for infection transmission. Cohorting minimises interactions between those who are infectious and those who are not.
Cohorting uses three risk categories:
- Confirmed infection – patients with the same confirmed pathogen are grouped together during the infectious period.
- Suspected infection – patients suspected to have an infection caused by the same pathogen are cohorted separately from those confirmed to have the infection and separately to those not suspected of having the infection.
- No identified infection risk – patients not suspected of having the infection, or those deemed to be cleared of a previous infection, are grouped together.
Staff caring for patients with suspected or confirmed infections, where possible, should be cohorted. Each cohort should be assigned to work with either suspected or confirmed patients to minimise the risk of transmission.
Zones
Zoning is a technique implemented to support cohorting within a facility. Zoning is relative to the size of the outbreak and layout of the facility.
Zoning may be difficult to apply in the residential care environment due to issues such as residents moving around the facility, but it remains important to consider how to apply zoning (in whole or in part) in the event of an outbreak.
Zoning may not be feasible in some accommodation settings such as supported independent living or group homes. In these settings, residents have their own room but may share bathrooms, meal and living areas. In evaluating suitability for zoning, consider the needs and behaviours of the patients, the physical layout of the home, and staff capacity to support zoning.
To remain prepared for COVID-19 outbreaks, health services must have an Outbreak Management Plan. A plan must include:
- identified areas that are suitable for use as COVID-19 clinical care zones
- colour coded or labelled floor maps outlining each zone
- instructions on how to implement and manage each zone.
Implementation of zoning requires a coordinated multidisciplinary approach. Zoning should be reviewed regularly, and adjustments made as required. Clear command structures, monitoring procedures and communication pathways should be established when zoning is implemented, scaled up, de-escalated, or stood down.
Zones may be:
- one room (single room isolation)
- a few rooms geographically co-located or separately located in the same area (ward/wing/building)
- an entire ward, wing, or building.
Table 4: COVID-19 care zones
| Zones | Description |
|---|---|
| Blue zone | This is an area between contaminated and non-contaminated zones. It is a staff-only area with no patient access, for example: nurses’ stations, staff tea rooms, meeting rooms, drug rooms, sterile stock rooms or office spaces. This zone may not be possible or necessary in areas that only include red and amber zones. |
| Green zone | This is a patient care area or administrative areas such as office and kitchen, where there are no people with suspected or confirmed COVID-19, and no people recently cleared of infection. |
| Amber zone | This is a patient care area with patients requiring quarantine, such as those identified as contacts. Patients in this zone should remain isolated from each other where possible and not congregate in communal areas. |
| Red zone | This is a patient care area used for isolation of patients with COVID-19. This zone may be a single patient room or multiple patient rooms in one area, or an entire ward. Patients have confirmed or suspected COVID-19. |
Considerations when setting up zones
When planning zones, consider:
- building layout and available space
- availability of single and shared rooms within the ward, wing, or building. Single rooms should be prioritised for patients with significant symptoms
- availability and location of bathrooms and toilets
- the ability of the patient/resident to remain in their room
- workforce capacity to support zoning
- placement of donning and doffing stations in each zone
- access to supplies (for example linen and other consumables) to enable easy access without crossing zones
- availability of mechanical ventilation, and capacity to increase natural ventilation.
Patients with suspected or confirmed COVID-19 should be placed in single rooms with their own bathroom, if possible. If single negative pressure ventilation isolation rooms are available, prioritise their use for patients who have higher transmission risk or who may require aerosol-generating procedures.
Zoning must be accompanied by a robust staff education and training program.
Amber and red zones should:
- be geographically separated from blue zones and green zones if possible
- be decluttered as much as possible. Items and equipment that are not frequently used should be put away in easy-to-clean storage containers, cupboards, or drawers
- have limited number of entry or access points. If possible, the entry and exit points for each zone should be separated and monitored.
Workforce
Cohort healthcare workers (HCWs), cleaning and catering staff and assign to one zone where possible. Staff should not work across red, amber, and green zones.
All clinical and non-clinical workers should be in line with current HCW COVID-19 vaccination recommendations; see Vaccination for healthcare workers.
All staff working in or entering red zones and amber zones should be trained and competent in the use of PPE, including correct donning and doffing procedures and fit checking. They should have undergone P2/N95 respirator fit testing.
During a surge, organisations should consider having additional staff above baseline numbers, for example:
- runners to support staff in red and amber zones by fetching items such as equipment and linen. This reduces the need for PPE changes
- trained PPE buddy or spotter to observe and support safe use of PPE
- cleaning staff to meet the increased cleaning and disinfection requirements
- staff to manage waste removal for all areas.
- in RCFs, an allied health or leisure and lifestyle staff member to provide activities for residents who are well enough and are in quarantine or isolation.
Considerations when assigning staff to a zone:
- the ability to meet patient care requirements, including for patients with challenging behaviours/behaviours of concern which may require additional staffing
- prevention of staff fatigue associated with frequent changing and prolonged time in PPE, which predisposes to breaches or mistakes
- separate staffing rosters for red and amber zones and non-COVID-19 (green) zones
- HCWs assigned to red and amber zones should be experienced, if possible. They should not simultaneously work in or be assigned to non-COVID-19 areas
- ensuring staff assigned to red and amber zones have skills in applying infection control principles and are competent with the use of required PPE
- the possible need to activate staff surge workforce as per pandemic or outbreak management plan, in response to a potential loss of 50% or more of the workforce.
Staff amenities
There should be no shared food, for example, no shared biscuit tins, fruit bowls, chocolates. Food should not be consumed in clinical areas.
Consider staggered meal breaks to reduce staff interaction. Consider recording or logging attendance in the tearoom.
Staff tea rooms must be in a blue zone.
A red zone should ideally have its own designated nursing stations, break areas and bathroom facilities which are not shared with staff from other zones. Consideration should similarly be given to separate outside fresh air and smoking/vaping areas.
If dedicated segregated staff break areas are not achievable, staff break areas should be organised in such a way as to promote physical distancing.
Staff bathroom and toilet facilities in a red zone or amber should not be used if there is no space for safe donning and doffing stations.
Staff returning early from quarantine should not take breaks with other staff.
Designate areas where staff can change out of their work uniform before leaving work if they wish to do so.
Zone entry, exit and traffic flows
Use demarcation signage or floor markings (if there is a lack of structural barriers such as doors) to identify the beginning and end of a zone.
If a zone is an individual room, use signage to identify the zone type and to support staff to select the required PPE.
Wherever possible, establish clear one-way and one-person-only direction of movement along corridors. If this is not possible, use floor markers to designate the desired direction of movement (for example, directional arrows on the floor with left side in and right side out).
When setting up PPE stations:
- Set up donning and doffing stations in areas with the least amount of foot traffic and with sufficient room to don or doff.
- There should be a minimum of 1.5 metres between donning stations, doffing stations, and the patient.
- Clearly mark donning and doffing stations using signage and/or floor markings.
- Assign a donning and doffing station to the entry and exit point of each zone.
Shared equipment
Equipment must be cleaned and disinfected between each use according to the manufacturer’s instructions.
- Amber zone – ideally, dedicated equipment should be allocated to each patient. Equipment may be shared within the zone following cleaning and disinfection.
- Red zone – ideally, dedicated equipment should be allocated to each patient. Equipment may be shared within the zone following cleaning and disinfection.
- Green zone – equipment may be shared within the zone following cleaning and disinfection
- Equipment that is used in amber or red should not be taken to a green zone.
Patient flows
Health services should have plans and procedures for:
- patient transfers in and out of red zones and amber zones. Consider internal transfer pathways including ambulance admission, emergency department, specialist diagnostics, operating theatres, and ward admission
- priority allocation of negative pressure and single rooms
- deteriorating patient pathway, that is, Intensive Care Units (ICU), operating theatres, endoscopy, and Coronary Care Units (CCU)
- provision of diagnostics at bedside, where practical. Have a transfer process in place for other diagnostic requirements, including specimen collection.
Managing surge
Where possible, patients/residents should be cared for in single rooms with their own bathroom. During surge periods with increasing numbers of COVID-19 cases, cohort isolation of confirmed cases in shared rooms may be considered.
Confirmed COVID-19 cases with another infection, such as influenza or multi-drug resistant organism colonisation, should be allocated a single room with a dedicated bathroom.
The number of confirmed cases that should be cohorted in one room should be based on the room’s capacity. It should be possible to:
- meet bed separation requirement of >2 metres, to accommodate staff movement and equipment and to ensure adequate air circulation
- maintain good air circulation by positioning clinical equipment to ensure that it does not impede airflow
- access an ensuite bathroom
- close doors to the room
- ventilate the room, preferably using a heating, ventilation and air-condition (HVAC) system
- maximise fresh air supply
- increase air exchange to create a negative pressure to adjacent rooms with consideration to exhaust through bathroom
- access individual ventilation hoods if appropriate for the patient population; for example, in ICU settings
- access portable air cleaning units to filter contaminated air
- consider patient/resident population risk factors, for example, aerosol generating behaviours or ability to follow instruction.
Health services should:
- plan for management of surges with increased numbers of presentations in Emergency Departments (ED and Urgent Care wards and the extension of SCOVID/COVID wards (that is, hospital in the home, home quarantine and alternative locations for the care of low-acuity COVID positive people)
- consider strategies for the establishment of ICU outside of established ICU wards (that is, use of operating theatre recovery areas) and management of open ICU wards verses those ICU wards that have single rooms. Prioritise single rooms for aerosol generating procedures
- consider strategies for assigning ventilators and supportive airway management strategies, for example, Continuous Positive Airway Pressure (CPAP)
- develop plans to de-escalate as patients recover or there are reduced number of admissions.
Personal protective equipment for zones
Standard and transmission-based precautions must be always followed. Single-use eye protection must be disposed of when removed. Reusable eye protection should be cleaned and disinfected according to the manufacturer’s instructions and stored clean, dry, and protected from contamination.
Table 5: PPE for zones
| Zone | Description |
|---|---|
| Blue zone | Respiratory protection as determined by organisational policy. |
| Green zone | Respiratory protection as determined by organisational policy. |
| Amber zone | COVID-19 airborne precautions, see section 4.1 – PPE when caring for patients with confirmed or suspected COVID-19 infection. |
| Red zone | COVID-19 airborne precautions, see section 4.1 – PPE when caring for patients with confirmed or suspected COVID-19 infection. |
Extended use of PPE* is permitted where all patients have the same risk as confirmed cases, and if the patient does not have another infectious condition. (*excluding gloves)
Note: In amber and red zones where there is a mix of confirmed and suspected cases, gowns (if worn) must be changed when moving from care of a confirmed case to care of a suspected case.
Release from isolation
Release from isolation should be considered in consultation with the infection prevention and control team, the treating medical team and where appropriate, the LPHU with reference to department guidance as relevant, see the department's COVID-19 (Coronavirus disease 2019) advice.
Further advice and guidance can be found at Coronavirus (COVID-19) – CDNA National Guidelines for Public Health Units.
Patients with COVID-19 who are discharged back to their home environment and health workers who have COVID-19 and are isolating at home should comply with current department advice on duration and conditions of isolation.
Hospitalised patients who are being transferred to another ward or hospital should remain in isolation with transmission-based precautions and appropriate PPE until criteria are met for release from isolation.
People who have recovered from COVID-19 and have been released from isolation based on the criteria above do not require COVID-19 testing if they are hospitalised for a non-COVID-19 related condition.
Patient transport
The transferring health facility should notify ambulance or other transport agencies on the patient’s condition and COVID-19 status to ensure all HCWs involved are aware of the PPE requirement prior to arrival.
All agencies involved in the transport of COVID-19 suspected or confirmed patients should implement their organisations' standard and transmission-based precautions.
Before transporting patients with suspected or confirmed COVID-19, perform a risk assessment on
- the type of vehicle required
- the physical capability of patient/client and whether assistance will be required
- the ability of the patient/client to wear a surgical mask and practice respiratory etiquette (hygiene).
Ideally no other patient should be transported at the same time (for example, no multi-loading). Exemptions to this approach can be applied with high community transmission and demand on the health service.
For suspected or confirmed COVID-19 patients, before entering the vehicle, the driver, clinician, and passenger should perform hand hygiene with ABHR. The driver should follow airborne precautions. Eye protection is not required for drivers as this may obscure vision.
Passengers should wear a surgical mask or respirator, perform hand hygiene, and be educated on respiratory hygiene. Passengers should be provided with a plastic bag, tissues and ABHR.
Whenever possible, drive with windows open and keep the vehicle fan on fresh air (not recirculation).
The vehicle should be cleaned at the end of the journey. Remove any visible contamination with detergent and disinfectant wipes. Clean the seat area, door handles, and any other high-touch areas or areas touched by the patient with detergent and disinfectant wipes.
Patient movement within a facility
Movement of confirmed and suspected COVID-19 patients within a facility should be limited to essential purposes.
If it can be tolerated, patients should wear a P2/N95 respirator or a surgical mask during transfer to another department within the facility. The receiving department should be notified of the patient's infectious status in advance.
Patient transfers within a health organisation should use a route that minimises contact with the general hospital population, including clinicians, for example, a dedicated lift or an external path.
5.3. Other IPC strategies
Physical distancing
Principles of physical distancing may be applied in any workplace setting (including non-healthcare settings):
- limit the number of people present in enclosed rooms
- maintain 1.5 metres distance from other people when feasible, except for the provision of direct care
- minimise time in close proximity, and wear a mask if 1.5 metres distance cannot be maintained
- position waiting room chairs 1.5 metres apart or block out interval chairs
- rearrange furniture to limit staff congregation in staff communal areas
- conduct staff interactions at a distance, for example, during ward rounds, shift handovers and meal breaks
- stagger break times to limit levels of staff congregation. Encourage breaks outdoors when possible.
In residential care settings, communal activities may still proceed if physical distancing is maintained. This may mean smaller groups are offered more frequently. During outbreaks, communal activities may need to be suspended.
Aerosol-generating procedures and behaviours
Aerosol-generating procedures (AGPs) may need to be performed during the care of patients suspected or confirmed to have COVID-19. Procedures that are believed to have a potential to generate aerosols or droplets include positive pressure ventilation, bilevel positive airway pressure (BiPAP) and continuous positive airway pressure (CPAP), endotracheal intubation, airway suction, high-frequency oscillatory ventilation, tracheostomy, chest physiotherapy, nebuliser treatment, sputum induction, and bronchoscopy.
Procedures that may cause aerosolisation of fluid or tissues that are not from the respiratory tract or lungs are not considered high risk AGPs for transmission of COVID-19.
AGPs should, whenever possible, be conducted in a negative pressure single room or a well-ventilated standard pressure room with a portable air cleaner. Personal ventilation hoods may be considered if a standard room is used.
Patient factors that increase the risk of COVID-19 transmission include aerosol generating behaviours such as:
- shouting or screaming
- coughing or increased work of breathing
- cognitive impairment or inability to cooperate
- refusing to wear, or inability to tolerate, a surgical mask.
Health care providers should complete a patient-centred risk assessment to determine the clinical need to complete AGPs. Consideration should be given to alternative therapy in consultation with treating medical team.
AGPs on suspected or confirmed COVID-19 persons should be performed with a minimum number of HCWs present and where possible, the most qualified person should carry out the procedure.
If feasible, CPAP, BiPAP or nebuliser therapy should be administered by the user themselves to reduce the risk of infection transmission to others. Only essential staff required for clinical care should be present during the procedure.
Airborne and contact precautions should continue to be used for the minimum settle time after the patient has left the room. The room should be left unused for a period after an AGP has been performed. A minimum settle or wait time of 30 minutes is recommended for negative pressure rooms, and up to 60 minutes for a standard room where the number of air changes per hour is not known.
If the number of air exchanges per hour is known, the minimum wait time can be calculated using the CDC Guidelines for Environmental Infection Control in Health-Care Facilities (2003). Airborne Contaminant Removal Table B.1 available at Centers for Disease Control and Prevention (CDC).
Cleaning and disinfection of the procedure room should be undertaken following an AGP except if the procedure is conducted in a designated isolation bedroom. Surfaces in rooms where CPAP, BiPAP or nebuliser therapy are performed should be cleaned and disinfected according to facility cleaning schedules.
While respiratory aerosols may have a wide dispersion range, many of the small droplets fall to the ground or surfaces within 1 metre of the user. In at-home care settings, enhanced cleaning and disinfection after each use should be focused on hard surfaces within an approximate 1 metre radius of where the therapies were performed, in addition to regular cleaning schedules.
Assisting with patient hygiene
Toilet flushing may generate microbe-containing aerosols. Toilet lids should be closed when flushing.
Indoor bathrooms are often poorly ventilated, so prolonged periods of time spent in these environments could increase the risk of infection transmission to carers and staff. Additionally, the wet conditions and humidity may dampen respirators and impair their function.
The risk assessment for showering should consider:
- the level of support or assistance required
- whether the room has sufficient ventilation
- whether the room has sufficient space to provide care without contamination to self
- whether the patient/resident has a clinical need for showering, is physically capable, and can cooperate.
While showering:
- use a face shield to protect the respirator from moisture splash or spray. Avoid getting the respirator wet
- turn on extractor fans while showering and leave the door open, if possible
- replace PPE after shower.
Alternative methods of providing personal hygiene care should be used when the risk of showering is deemed unacceptably high.
Medical records and patient charts
The risk of contamination of paper health records and subsequent exposure to COVID-19, in the absence of a spill (or similar), is considered extremely unlikely and negligible risk.
Standard precautions apply to the management of all patient charts and medical records. Patient charts and records should remain outside patient rooms.
PPE must be removed, and hand hygiene performed before writing on paper charts or medical records.
Medical records do not need to be quarantined before being returned to health information services.
Outbreak response kits in RCFs
An outbreak response kit should be prepared before any potential outbreak. It should be accessible for staff to use immediately if there is an outbreak.
The kit should include essential documentation that will allow the immediate implementation of an outbreak response:
- the facility’s outbreak management policy and guidelines
- a checklist of essential tasks and notification pathways
- contact details (all hours) of the internal outbreak notification pathways
- contact details (phone/email/weblink) for external outbreak notification
- the cohort and zoning plans for the unit
- outbreak signage.
It should also include equipment and consumables:
- large wipeable container with lid to store kit contents. Consider sealing the kit when not in use to prevent ad hoc use of the outbreak start-up stock.
- surgical masks
- P2/N95 respirators
- impervious / fluid repellent gowns
- nitrile / latex gloves in L, M and S sizes
- protective eyewear: goggles / face shields.
Consider the need for ready access to:
- a supply of large general waste bins and bin liners
- chemical disinfectant approved by the Therapeutic Goods Administration; see Disinfectants for use against COVID-19 in the ARTG for legal supply in Australia.
When deciding how much stock to keep in the kit, consider the facility size, number of residents, and the time that any new orders of stock would take to be delivered.
For more information see:
- COVID-19 self-assessment tool for residential aged care facilities
- COVID-19 self assessment tool for residential community and disability services
- COVID-19 self assessment tool for non-residential community and disability services
Care of the deceased
Care of the deceased should follow the health service guidelines and relevant legislation. Routine occupational health and safety guidelines and infection control procedures apply to the management of deceased bodies, with the same precautions in place after death as were in place prior to death.
COVID-19 standard and transmission-based precautions continue to apply when handling the body. At a minimum, contact and droplet precautions should be used.
Avoid unnecessary manipulation of the body that may expel air or fluid from the lungs. Airborne precautions are required if there is a risk of generating aerosols, for example in post-mortem extubation or procedures involving high speed devices.
HCWs handling deceased bodies should wear appropriate PPE: apron/gown, gloves, masks, and face shield/goggles.
If a family member touches the body, they should wash their hands with soap and water immediately afterwards or use ABHR.
When transporting the deceased, the body must be placed and secured in a body bag or wrapping in a manner that prevents the leakage of body fluid or other substance. Double bagging may be required to achieve this.
5.4. Visitor and family strategies
Health services should employ local risk assessments to determine any restriction to visitor numbers or testing requirements, noting that there may be areas of a health service where visitor restrictions may need to be applied.
Visiting suspected or confirmed COVID-19 cases
Visiting a person with suspected or confirmed COVID-19 presents a considerable risk of transmission. The decision to allow visitors to a patient suspected or confirmed to have COVID-19 should be managed on a case-by-case basis in conjunction with the treating medical team and the health service Infection Prevention and Control team. Refer to Department and LPHU guidance as relevant.
It is particularly important for facilities to assist visitors to visit safely. Visitors must use the same PPE protection and infection prevention practices as healthcare workers. Staff should provide instruction, assistance and supervision of PPE selection and use by visitors.
Family as carers in residential care facilities (RCF)
A carer model may be implemented as a continuity of care strategy and for compassionate reasons during an active COVID-19 outbreak at an RCF.
One relative or usual carer per resident may be designated as an Essential Carer (EC) and may be permitted to provide care to their resident on-site at the facility.
For more information see:
Ventilation
Guidelines for optimising ventilation to reduce the risk of transmission of COVID-19 in healthcare settings.
Ventilation of indoor spaces provides air that will assist in the dilution and dispersion of smaller particles in the air (for example, dust, pollen and microorganisms) and improve overall air quality.
Ventilation of a space can be provided either mechanically (for example, via a centralised heating, ventilation and air conditioning (HVAC) system or an individual local air conditioning unit) or naturally with passive airflow. Ventilation can also be augmented by filtration.
Ventilation should be considered as part of a group of IPC strategies to reduce the risk of COVID-19 transmission in workplaces. For more information, see Better Health Channel's Improving ventilation to stop the spread of COVID-19.
Poorly ventilated spaces can increase the risk of infectious respiratory particle transmission. It is strongly recommended to optimise ventilation in indoor settings to protect the most vulnerable.
Further information is available at Australian Commission on Safety and Quality in Healthcare, Optimising ventilation for infection prevention and control in healthcare settings.
6.1. Air changes per hour (ACH)
Ventilation air change rate is typically measured in air changes per hour (ACH). ACH refers to the number of times the volume of air in a space is completely replaced per hour. Evidence suggests that air change rates of 4-5 are good, 6 is better and more than 6 is best. Aim for 5 or more ACH to help reduce the number of viral particles in the air. Air change can be achieved through any combination of natural ventilation, mechanical ventilation, or devices that augment existing ventilation systems.
While the 5 ACH target is a rate that is likely to be helpful in reducing infectious particles, an optimum number of ACH remains uncertain. ACH levels higher than 5 may remove infectious aerosols from a space faster, but the potential benefits should be balanced with the additional upfront cost, and the costs of periodic maintenance, comfort level, and energy costs that will be incurred.
In standard hospital rooms, a minimum of 6 ACH is required. In negative-pressure isolation rooms, 12 ACH is required. Large volume spaces with very few occupants (e.g., a warehouse) may not require 5 ACH and spaces with high occupancy or higher-risk occupants may need higher than 5 ACH.
For guidance on calculating ACH, see Centres for Disease Control and Prevention (CDC) May 2023, Ventilation in Buildings.
6.2. Types of ventilation
Natural ventilation
Natural ventilation uses natural wind and thermal air differences to bring fresh air (outdoor air) into a space. Natural ventilation is passive outside air flow via openings such as windows, doors and air vents.
The ventilation rate in naturally ventilated spaces can vary significantly throughout the year due to changing weather patterns and unfavourable conditions (for example, temperature, wind and rain) which may cause occupants to open or close windows and external doors sporadically.
Natural ventilation is significantly better than no ventilation, in most circumstances. However, if mechanical or augmented ventilation is available, these may be preferred due to the following risks associated with natural ventilation:
- airflow depends on wind currents, so the rate of ventilation cannot be controlled
- air is not filtered, so there is a risk of exposure to poor quality air, dust and other contaminated airborne particles
- temperature is not controlled, so external environmental conditions such as rain, humidity and heat can reduce patient and staff comfort
- unfiltered air and uncontrolled temperature and humidity may breach specified conditions for storing sterile stock
- when used in combination with mechanical systems such as split systems, natural ventilation may reduce the system’s temperature control and depending on outdoor conditions, may increase condensation levels. This will increase system running costs.
Mechanical ventilation
Mechanical ventilation replaces or dilutes indoor air with outside air using mechanical equipment (for example, HVAC systems). Conventional HVAC ventilation systems dilute indoor, potentially contaminated air through the introduction of fresh air from the outside while maintaining indoor air quality (IAQ) and thermal comfort.
Ventilation systems are not designed to prevent COVID infection transmission but to meet requirements to control the accumulation of harmful contamination and provide occupant comfort. A well-maintained and appropriately designed HVAC system contributes to the diffusion and dilution of infectious aerosols, reducing the risk of infection transmission.
HVAC systems
Centralised heating, ventilation, and air conditioning (HVAC) systems dilute indoor, potentially contaminated air through the introduction of fresh air from the outside while maintaining indoor air quality (IAQ) and thermal comfort.
A well-designed, located and maintained HVAC system can reduce respiratory particle transmission by:
- supplying clean air to areas where susceptible occupants are located
- containing contaminated air and/or exhausting it to the outdoor environment
- diluting the air in a space with cleaner air from outdoors and/or by filtering the air of aerosols.
Most ventilation systems are designed for thermal comfort, not for preventing the transmission of infection. However, a well-maintained and appropriately designed HVAC system will contribute to the diffusion and dilution of infective respiratory particles, reducing the risk of infection transmission. The system should be well-maintained and serviced as per regular schedules.
Improving ventilation and airflow in indoor settings using an HVAC system should be considered as part of a suite of infection control measures to mitigate COVID-19 transmission risk.
The settings on an HVAC system can be adjusted to maximise ventilation. This needs to be done by a HVAC specialist or an occupational hygienist.
Split system air conditioners
Split system air conditioners (split systems) usually consist of two mechanical units:
- an indoor unit that provides conditioned air into a space (containing heat exchange coils, filters, fan)
- an outdoor unit that transfers refrigerant to and from the indoor unit (contains the compressor, propeller fan, circuit board and heat exchange coils).
Multi-split systems have more than one indoor unit connected to a single outdoor unit. They are used to heat or cool different spaces or rooms.
Ducted split systems have a single outdoor unit connected to a concealed indoor unit, which is then ducted to a single or multiple rooms.
Split systems recirculate air and promote air movement, but usually do not bring fresh air into a space unless specified (for example, unless they are designed to include outdoor air provision). Split systems should be used in conjunction with mechanical or natural ventilation to promote air movement and to minimise pockets of stagnant air. They are not a replacement for natural or mechanical ventilation.
Evaporative cooling
When in use, evaporative cooling systems bring in large quantities of air from outside achieving very good air change rates. Some windows or doors need to be left open for these systems to circulate fresh air effectively.
Run evaporative coolers or ducted systems once or twice a day in ‘fan-only’ mode to flush rooms with fresh outside air.
Evaporative cooling systems need to be serviced regularly to make sure they are running effectively, and the filter changed regularly according to the manufacturer’s instructions.
It is important to note that evaporative cooling systems will only be useful during the warmer periods of the year and are unlikely to be used during the cooler months.
Augmented ventilation
This refers to supplementary devices to improve existing natural or mechanical ventilation.
These can assist in:
- reducing the concentration of aerosolised viral particles
- improving air circulation and distribution in a space to reduce dead spots.
Augmented ventilation does not provide outdoor air to a space and is not considered an appropriate substitute for natural or mechanical ventilation strategies.
Augmented ventilation should aim to contribute to 5 or more ACH of clean air in the space to help reduce the risk of airborne infection transmission.
6.3. Air cleaning
Filtration
Filters are designed to remove particles from air streams as they pass through. The Minimum Efficiency Reporting Value (MERV) is a scale for the measurement of an air filter’s ability to capture particles between 0.3 to 10 microns (µm) as air passes through. MERV filters range from 1 to 16, the higher the rating, the smaller the particles they capture (the more efficient they are). The minimum recommended filter is MERV ≥ 13; these filters are cost efficient compared to higher MERV rated filters, and are efficient at capturing airborne viruses.
Upgrading filters to those with ratings of MERV 13 or higher will reduce the transport of airborne particles while systems are operating, which may help reduce airborne infectious disease transmission within rooms and between rooms.
H13 grade high-efficiency particulate air (HEPA) filters are efficient at filtering larger than 0.3 µm diameter particles in standard tests. Particles larger than 0.3 microns include pollen, pet dander, dust, mould spores, smoke and bacteria as well as aerosols.
Air disinfection
Ultra-violet (UV) light can be used as a supplemental treatment to inactivate airborne viruses such as SARS-CoV-2 in some indoor environments. UV disinfection has been used in some high-risk healthcare settings to prevent and control respiratory disease transmission. It supplements other ventilation strategies as it can reduce airborne virus concentrations in indoor spaces. However, it does not increase air exchange rates or remove particles from the air. For more information, see section 6.5. Air treatment with germicidal ultraviolet (GUV).
Portable air cleaners
An air cleaning device is a portable air circulator which draws air through a series of filters to remove particles before releasing cleaned air. Air cleaning devices can recirculate air back into a room or be ducted to exhaust air to the outside. Air cleaners can be used to increase the air exchange in a space and increase clean air change rate when used appropriately. The use of air cleaning devices can be considered in:
- workplaces with low ventilation rates despite implementation of natural and mechanical ventilation; or
- settings with elevated risk of COVID-19 infection transmission.
Position portable air cleaning devices so that air intakes are clear of obstructions. Most air cleaning devices draw air in from the front so that you can position them near a wall or in a corner, to promote good air movement. Portable air cleaning devices should be positioned with a small amount of space around the sides and the back.
Position air cleaning devices:
- away from open doors and windows
- in areas of low movement (‘dead spots’); often in corners or the points furthest away from any door and window openings
- in corners or dead spots to aid air circulation
- near supply grilles, where possible, to aid circulation of the filtered air
- to ensure that they do not create trip hazards, such as from loose cables
- to ensure that they do not obstruct entry and exit paths, such as fire exits.
Portable air cleaning devices should not be positioned near open windows or underneath extract grilles. Do not place objects on top of air cleaning devices.
For information on purchasing air cleaners, see 'Purchasing an air cleaner' under section 8.5. in References.
6.4. Fans
Like split systems, electrical fans (including portable pedestal, box and fixed ceiling fan types) can circulate air in a room and promote air movement in a space, but do not provide fresh air. Air currents and movement provided by fans can encourage dilution and even distribution of particles (including viral particles).
If there are existing mechanical and natural ventilation strategies in place, fans may be used to encourage even air distribution. Pedestal or portable fans should ideally be placed in dead spots or areas with poor airflow, avoiding a potential build-up of viral particles in this area. Windows and doors should remain open where possible. A fan can be placed in front of an open window (facing to the outside) to increase air flow by pushing indoor air outside.
Fans should not be used if someone in the space has respiratory symptoms that are consistent with COVID-19 or is suspected or confirmed to have COVID-19. Once the person has left the space, fans may resume operation. Fans should not be directed to blow air from one person directly onto another person.
You should also:
- avoid the use of the high-speed settings
- use ceiling fans at low velocity
- direct the fan discharge towards an unoccupied corner and wall spaces or up above the occupied zone
- position portable or pedestal fans:
- in areas of low movement (‘dead spots’), often in corners or the points furthest away from any door and window openings
- in corners or dead spots to aid air circulation
- to ensure that they do not create trip hazards, such as from loose cables
- to ensure that they do not obstruct entry and exit paths, such as fire exits.
6.5. Air treatment with germicidal ultraviolet (GUV)
GUV can be used as a supplemental treatment to inactivate airborne viruses, such as SARS-CoV-2. GUV can be effective in many spaces, but it can be especially useful as an additional layer of protection to reduce infectious particles in indoor spaces that host large gatherings or where the risk of disease transmission is high. Historically, UV aerosol disinfection has been used in high-risk healthcare settings to prevent and control respiratory disease transmission.
Installation of UV disinfection devices requires careful consideration and extensive professional consultation for a range of factors, such as occupational health and safety, material durability and design of space.
Upper-room (or upper-air) GUV uses specially designed GUV fixtures mounted on walls or ceilings to create a treatment zone of ultraviolet (UV) energy that is focused up and away from people. These fixtures treat air as it circulates from mechanical ventilation, ceiling fans, or natural air movement. The advantage of upper-room GUV is that it treats the air closer to and above people who are in the room.
In-duct GUV systems are installed within a heating, ventilation, and air conditioning (HVAC) system.
These include:
- coil treatment GUV to keep HVAC coils, drain pans, and wetted surfaces free of microbial growth. These devices produce low levels of UV energy. This energy is continually delivered 24 hours a day, which is why they are effective.
- air treatment GUV systems which apply intense UV energy to inactivate airborne pathogens as they flow within the HVAC duct; however, air speed must be slow enough to allow adequate exposure to UV.
HVAC air treatment GUV systems require more powerful UV lamps or a greater number of lamps, or both, to provide the necessary GUV required to inactivate pathogens in a short period of time.
Air treatment systems are often placed immediately downstream of the HVAC coils. This location keeps the coil, drain pan, and wetted surfaces free of microbial growth and treats the moving air.
Standard GUV systems are designed to avoid exposing people to injury caused by direct exposure to UV energy.
6.6. Ventilation indicator devices (CO2 monitors)
Carbon dioxide (CO2) monitoring can provide information on ventilation in a space. Changes in CO2 concentration can indicate a change in room occupancy and the amount of outdoor air delivered can be adjusted.
However, there is not a direct link between CO2 concentration and the risk of COVID-19 transmission. CO2 concentration cannot predict if one or more room occupants has COVID-19 infection, the amount of airborne viral particles produced by infected people, or whether the HVAC system is effective at diluting and removing viral concentrations near their point of generation.
Nonetheless, a CO2 concentration below 900 parts per million (ppm) can be used as an indicator of good ventilation. It is important to note, however, that this concentration may not be appropriate for assessing the ventilation of all types of spaces and occupancies.
There are other methods of monitoring and remote sensing including monitors of pollution, volatile organic compounds (VOCs), carbon monoxide, temperature and other air contaminants. There are also options which allow information to be viewed in real time on a dashboard.
For more information on indoor CO2 recommendations refer to:
- Australian Building Codes Board, Handbook: Indoor Air Quality
- Australian Standards, AS 1668.2
- Centres for Disease Control and Prevention (CDC) May 2023, Ventilation in Buildings
6.7. Activities and devices that move air
The following devices and activities can create air currents or turbulence which may disperse aerosols.
Hand and hair dryers
These are safe to use and unlikely to contribute to the spread of COVID-19.
Vehicle air conditioning
When in a shared vehicle, the heating and air conditioning system should be turned to fresh air mode (not recirculated air) to bring fresh outdoor air into the car. Windows should be kept open when practicable.
Singing and music in group settings, such as choirs and wind instruments
During singing and playing of wind instruments, droplets and aerosols are emitted and can follow ambient airflow patterns in a space. If a person is infectious, they may transmit COVID-19.
Measures that may reduce the risk of infection transmission include:
- singing or playing outside or in a well-ventilated room
- physical distancing between singers or players
- collecting and disposing of condensation and saliva hygienically
- performing hand hygiene after playing musical instruments
- cleaning surfaces between each use.
E-cigarettes and vaping devices
It is recommended that people maintain a 2 metre distance from a person who is vaping or smoking.
The frequent hand-to-mouth action and sharing devices with others may increase the risk of infection. Hand hygiene should be performed before and after using the device.
6.8. Ventilation strategies for acute healthcare settings
Ventilation cannot be considered as a sole infection control measure but should be used in conjunction with other infection control strategies. All acute healthcare services must undertake a risk assessment and planning for a range of ventilation and air-cleaning strategies to prevent COVID-19 transmission.
Ventilation and air cleaning strategies include:
- barrier air flow – the air flow from a COVID-19 patient’s room (hospital isolation room) or from a COVID-19 patient ward/zone (single rooms, or shared isolation areas used for the care of suspected and confirmed COVID-19 patients) should be actively ducted to the atmosphere outside of buildings and maintained at negative pressure (for example, clean air flows into the room passively and contaminated air is extracted out).
- filtration – to remove any suspended respiratory particles that may return to the air handling unit. F8 or F9 (ideal) filters are examples.
Isolation rooms and air changes per hour
Patients with confirmed or suspected COVID-19 should be cared for in a negative-pressure isolation room (preferable) or a standard-pressure single room.
Isolation rooms should include self-closing doors, an ensuite bathroom, high quality sealing of the room, an anteroom, independent supply air and exhaust, and exhaust ducts under negative pressure within the building.
In standard hospital rooms, a minimum of 6 ACH is required. In negative-pressure isolation rooms, 12 ACH is required.
Toilet and bathroom ventilation in isolation rooms
Toilet and bathroom ventilation systems should be kept at negative pressure and continuously run, 24 hours, 7 days a week if possible. Shower steam and toilet flushing may potentially cause aerosolisation of existing viral particles in the bathroom environment. Toilet windows are not recommended to be opened. This ensures correct ventilation direction and maintain negative pressure.
Natural ventilation
Natural ventilation should only be used if mechanical ventilation is not possible or available. This is because the natural airflow rate depends on window size and variable weather and may not quickly remove airborne particles. However, in healthcare facilities with no mechanical HVAC systems, natural ventilation is superior to no ventilation at all.
HVAC system maintenance and engineering support
All maintenance staff should wear appropriate PPE. Facility engineers should monitor and record the HVAC system metrics and the negative-pressure function of rooms in control zones daily. Bedside nurses should also monitor these and check whether alarms are working as part of their handover.
Scheduled maintenance should be reported to the infection control team quarterly (every 3 months). Air movement may also be mapped on an ad hoc basis, for example, using a smoke stick to determine air flow direction.
Hospital engineers should play a key role in reducing disease transmission in healthcare facilities. Their roles may include but are not limited to:
- ensuring, whenever possible, that all facilities are up-to-date with the latest practice standards
- creating new healthcare facility designs, including key points of entry such as emergency, admission and waiting rooms, incorporating the appropriate infrastructure including HVAC systems that separate high-risk areas; enough physical space and HVAC system capacity to upgrade filtration; the ability to increase ventilation to 100% outdoor air; and the ability to humidify air
- providing the capacity for quick installation of improved HVAC filtration
- providing the capacity for rapid, temporary increase in the outdoor ventilation rate in the event of an infectious disease outbreak.
- actively managing competing priorities to improve environmental outcomes through appropriate mitigation strategies.
For minimum maintenance schedules for air handling systems, see Maintenance standards for critical areas in Victorian health facilities.
Table 8: Ventilation strategies
| Strategy | Key actions checklist |
|---|---|
| Air exchanges per hour (ACH) | Standard pressure hospital rooms should have a minimum of 6 ACH. Negative pressure and quarantine isolation hospital rooms (with airborne respiratory virus infections) should have at least 12 ACH. |
| Negative pressure isolation rooms | Air flow from a COVID-19 patient’s room should be actively ducted to outside the building. Maintain independent supply air and exhaust to prevent recirculation and ensure clean air entry into the room. Exhaust ducts should be under negative pressure within the building. Should have: 12-15 ACH or 145L per second; doors that remain closed, high-quality sealing; an anteroom; differential pressure gauges outside the room; local alarm systems to monitor fan status; low level exhaust; and clinical handbasin. |
| Filtration | Install a minimum F8 or F9 (ideal) multi-pocket or V bank filter in the AHU as main filter. Minimum filtration grade MERV 13-16 (F8 or F9) is recommended. Consider HEPA filtration where existing system performance can be maintained. |
| Air circulation | Switch off or minimise air recirculation. |
| Barrier air flow (controlled volumetric air movement) | Change balance of supply air to extract air at the air handling unit (AHU) within a zone either by: - adjusting the fan speed via a variable speed drive - adjusting the volume control damper positions at the AHU Increase supply air into adjacent zones to force air towards designated COVID red zones. Maintain low differential pressure between control zone and adjacent space (in the order of -2 to -5 pa). Total air movement should be 150-200 l/s/double door into the zone. |
| Dilution ventilation | Maximise the use of outdoor air as reasonably possible (100% outdoor air is preferable). |
| Temperature and humidity | Maintain relative humidity and temperature limitations and controls set by the healthcare facility. |
| Natural ventilation | Not considered an adequate method to mitigate airborne transmission within healthcare facilities. Should not be considered unless that is the only viable ventilation option. |
| System maintenance | Label any HVAC systems set to pandemic mode. Monitor and record HVAC system metrics daily. Minimum maintenance requirement. Appropriate PPE should be worn by all staff and operators during maintenance work. |
| Onsite support provided by hospital engineers | At the building level, hospital engineers may identify: - vulnerabilities with air intake, wind direction, shielding etc. - building systems and safety zones in the general building environment. - approaches to interrupting air supply to designated ‘shelter-in-place’ locations in general building environments. - cohorting possibilities for pandemic situations so that whole areas of a hospital may be placed under isolation and negative pressure. |
| Other important considerations | Ensure all doors are always closed where appropriate. Avoid crowding. Utilise zoning. Utilise negative pressure rooms for confirmed COVID-19 patients and AGPs. Avoid non-essential emission sources such as burning incense. Be aware of corridor HVAC returns: wards with corridor return ducts move air from patient rooms through the corridor towards the return duct. |
6.9. Ventilation strategies for residential care settings
Whenever possible, these strategies should be implemented in consultation with an occupational physician or ventilation professional.
In red zones (see under section 5.2 'Isolation, cohorting, zoning' on Managing staff, visitors and outbreaks), the air should be actively ducted to the atmosphere outside the buildings.
The supply of outdoor air to HVAC systems should be increased as much as reasonably possible in all areas of the facility.
Where an HVAC system recirculates air between different rooms, this recirculation should be turned off to rooms housing people with confirmed or suspected COVID-19.
Installation of standalone air conditioning units or placement of air cleaning devices (air scrubbers, air filters and air purifiers) with HEPA filtration should be considered to improve ventilation in areas housing people with suspected COVID-19. However, consultation with an occupational physician or ventilation professional should be undertaken and a risk assessment or needs analysis should also be considered.
If the ventilation rate cannot be increased mechanically, or if the recirculation mode cannot be improved or changed, natural ventilation strategies can be adopted. These include:
- opening windows if it is safe to do so (this should only be considered if outdoor temperatures are comfortable or if the room is vacant)
- creating new openings by modifying doors or windows
- installing air extractors or whirlybirds to enhance the effects of other ventilation strategies.
The usual indoor temperature and humidity set points should be maintained. Resident and staff thermal comfort and safety should be prioritised. If an HVAC system has humidity control, the relative humidity should be kept at 40 to 50%.
Facilities should consider the comfort of residents and HCWs when in PPE for prolonged periods.
Where possible, residents should be cared for in single rooms with their own ensuite bathrooms.
Ventilation or exhaust fans in bathrooms should operate at all times in bathrooms of people who are confirmed or suspected to have COVID-19.
In amber and red zones, portable fans are discouraged because air currents may accelerate airborne transmission of aerosolised viral particles. When fans are unavoidable, they should be placed in locations where fan air flow will not be directed from one person directly towards another and where possible in front of an open window (facing to the outside) to increase air flow and push indoor air outside.
In blue and green zones, portable fans are safe to use.
In amber and red zones where there are no other viable alternatives to maintain ventilation within the space, ceiling fans may be used with caution, they should operate at the lowest setting with the door closed if possible.
Specific healthcare settings
Guidelines for preventing and controlling COVID-19 in primary and community care settings, COVID-19 testing clinics and other specific healthcare contexts.
This guidance is in addition to other IPC advice in these guidelines.
7.1. Primary care and community settings
Primary care and community settings include services provided in:
- Primary and community health settings and professional clinics, including medical/general practice, pharmacy, dental, nursing, allied health, day programs and social services.
- Residential dwellings (private homes and group housing) such as home-based care services including nursing, mental health, allied health, disability support, and social services.
- Institutional settings such as schools (sick bays, boarding schools), camps, disability housing, group housing, mental health facilities, youth housing, detention, youth justice, justice, or police and correctional facilities.
All community services staff, contractors and volunteers must wear appropriate PPE and follow IPC principles. Health workers required to use P2/N95 respirators should be fit tested and trained in correct respirator use, including completing a fit (seal) check every time a respirator is put on.
Services should complete a pre-consultation risk assessment (by telephone, telehealth, online meeting, or a screening station at the entry). Consider COVID-19 risk related to the client, environment, staff, and other people present.
General principles:
- face masks are recommended when visiting or working in sensitive settings
- minimise the number of people present during the interaction to those essential to the consultation
- maintain 1.5-meter physical distancing unless closer contact is essential to the interaction
- maximise ventilation and/or fresh air flows with open doors or windows where possible
- minimise and remove all items not essential to the consultation
- limit the number of people in clinics and waiting rooms to maintain physical distancing measures
- minimise contact during check-in
- on presentation, complete COVID-19 pre-screening for symptoms of COVID-19. If clinically appropriate, consider alternative appointment arrangements for:
- clients with ARI
- close contacts of known positive cases (until isolation period ends)
- clients with COVID-19 who are still in their infectious period
- use transmission-based precautions when COVID-19 risk has been identified
- establish donning and doffing stations in convenient and protected locations
- consider preparing designated rooms for high-risk interactions/clients.
When entering residential settings, in addition to the above:
- before entry, check the COVID-19 risk of the client and others who will be present during the interaction
- ensure you have resources for cleaning/disinfecting equipment, donning and doffing, and clinical waste bins or bags for PPE
- take only those items essential for the consultation into the home
- limit time inside the home
- ensure all items taken into residential dwellings are cleaned and disinfected when taken out.
7.2. COVID-19 testing clinics
If establishing drive-through, pop-up or mobile van COVID-19 testing clinics, it is important to consult with the local infection prevention and control team and to consider a range of infection prevention and control practices as follows.
Physical set up
When planning the location and workflow of a clinic, consider:
- ventilation of enclosed clinics (established or temporary building or a pop-up tent)
- physical distancing of >1.5 metres wherever possible
- signage to direct and inform patients, control traffic and queues, limit speed, etc.
- separate areas for staff to don and doff PPE safely
- allocated PPE-free zone for a staff break area
- separated and enclosed storage for both used and reprocessed items, for example, shared patient equipment and PPE. All reusable equipment/items must be reprocessed as per manufacturer’s instructions
- waste collection areas
- access for pathology couriers to collect specimens.
The clinic will need supplies of this equipment and consumables:
- ABHR
- equipment for specimen collection and security of specimens
- PPE for standard and transmission-based precautions, including uniforms
- products for routine and enhanced environmental cleaning
- products for cleaning shared patient care equipment (including chairs) after each use
- patient information resources.
Staffing
Staff will need:
- orientation and an education program on infection prevention and control
- training to enable good practice in taking swabs and enough resources to allow for practice.
Collecting specimens
When collecting respiratory specimens, transmission-based precautions for COVID-19 should be observed whether respiratory symptoms are present or not. Consider the need for eye protection following a risk assessment.
7.3. Aquatic facilities
There is no evidence that COVID-19 can spread directly to humans from water in treated aquatic facilities. Proper operation, maintenance, and chemical disinfection should destroy the virus. For hydrotherapy practices, conduct risk assessments of clients and staff to reduce risk.
7.4. Companion animals
The Australian Department of Agriculture, Water and the Environment have assessed that there is currently no evidence of transmission of COVID-19 to or from domestic animals – either pets or livestock. The current spread of COVID-19 is driven by human-to-human transmission. The use of therapy animals in the healthcare setting is therefore considered safe.
COVID-19 Infection Prevention and Control Guidelines References
Further COVID-19 information and resources for healthcare settings, including acronyms and abbreviations, a glossary of terms, mask and respirator standards and IPC education.
8.1. Acronyms and abbreviations
| Acronym | Description |
|---|---|
| ABHR | alcohol-based hand rub |
| aBL | antiviral blue light |
| ACH | air changes per hour |
| AGB | aerosol-generating behaviour |
| AGP | aerosol-generating procedure |
| ACIPC | Australian College for Infection Prevention and Control |
| ACSQHC | Australian Commission for Safety and Quality in Health Care |
| ARI | acute respiratory infection |
| BiPAP | bilevel positive airway pressure |
| CDC | Centres for Disease Control and Prevention (United States of America) |
| CDNA | Communicable Diseases Network Australia |
| COVID-19 | Coronavirus disease 2019 |
| CPAP | continuous positive airway pressure |
| ED | Emergency Department |
| EPA | Environmental Protection Authority Victoria |
| GP | general practitioner |
| HEPA | high efficiency particulate air |
| HVAC | heating, ventilation, and air-conditioning |
| HCW | healthcare worker |
| ICEG | Infection Control Expert Group |
| IPC | infection prevention and control |
| LPHU | Local Public Health Unit |
| NHMRC | National Health and Medical Research Council |
| NEPT | non-emergency patient transport |
| PCR | polymerase chain reaction (test for COVID-19) |
| PPE | personal protective equipment |
| RCF | residential care facility (includes RACF) |
| RACF | residential aged care facility |
| RAT | rapid antigen test |
| SARS-CoV2 | severe acute respiratory syndrome coronavirus 2 |
| SCOVID | suspected COVID-19 |
| TGA | Therapeutic Good Administration |
| WHO | World Health Organisation |
8.2. Glossary of terms
| Term | Definition |
|---|---|
| Aerosol-generating behaviour (AGB) | Behaviours that are more likely to generate higher concentrations of infectious respiratory aerosols such as persistent or severe coughing, screaming, or shouting, or heavy breathing and panting during active labour. |
| Aerosol-generating procedure (AGP) | A procedure that is more likely to generate higher concentrations of infectious respiratory aerosols, such as bronchoscopy, tracheal intubation, non-invasive ventilation (for example, BiPAP, CPAP), high-flow nasal oxygen therapy, manual ventilation before intubation, intubation, cardiopulmonary resuscitation, suctioning, sputum induction, and nebuliser use. Collection of nose and throat swabs is not considered an AGP. |
| Air cleaner/air scrubber/air purifier/air filter | A portable device which filters air to remove particles. |
| Clean air change rate (ACH) | The rate at which clean air volume is moved into and out of a space within an hour. This is measured in air changes per hour (ACH). |
| Cohorting (also see zoning) | Grouping individuals with the same condition or same laboratory-confirmed infection in the same location (a room, ward section or building). |
| Contact | A person at increased risk of contracting a transmissible disease due to exposure to an infected person. Contacts may be 'close contacts' which are also known as 'household contacts'; social contacts include workplace and education contacts. |
| COVID-19 | The disease caused by SARS-CoV-2. |
| Dead spot | In an enclosed space, an area where there is very little or no air movement. In these areas, any virus-laden aerosols could remain suspended in the air for prolonged periods of time. |
| the department | The Victorian Government Department of Health. |
| Fomite | An inanimate object that has been contaminated with an infectious agent. |
| HVAC (heating, ventilation, and air conditioning) systems | Centralised conventional ventilation systems that maintain thermal comfort by heating or cooling and introduce fresh air from the outside. The fresh air dilutes or replaces potentially contaminated indoor air. |
Negative pressure isolation room (Class N) | A room in a hospital or other facility used for patients requiring airborne isolation. In addition to being at negative pressure, the room may have additional barriers such as an anteroom. |
| Patient | The term ‘patient’ is used inclusively to refer to all consumers of health care services, including patients, residents, customers, clients and guests in healthcare, residential aged care homes, supported residential settings, primary and community care settings and clinics. |
| Personal ventilation hood | A hood over a patient’s bed providing a negative pressure environment that reduces the risk of aerosol transmission to healthcare workers. It consists of a plastic canopy over a frame, a HEPA filter, and an exhaust fan. |
| Residential care facility | Any public or private accommodation facility where residents sleep, eat and live either temporarily or on an ongoing basis. This includes residential aged care facilities (including nursing homes and hostels), residential care facilities for people with physical and cognitive or behavioural disabilities, and other similar accommodation settings. |
| SARS-CoV-2 | The causative virus for COVID-19. |
| Self-isolation | Separation from other people, including those in the same household, to stop the spread of a transmissible disease. |
| Source control | A preventative strategy for reducing airborne contaminant levels in the air, for example, by using a mask to prevent the release of respiratory particles from an infected person. |
| Ventilation rate | The amount of outdoor air that is introduced into a space. It is measured in m3/hr (cubic metres per hour), l/s/p (litres per second per person) or ACH (air changes per hour). |
| Viral emission rate | The number of viral particles expelled by an infected person over a particular unit of time. |
| Whirlybird | A wind-driven turbine located on a roof to improve extraction of air from a building. |
| Zones (also see cohorting) | Zoning means designating a room, wing, ward, floor or building to accommodate single and cohorted groups of patients who have the same transmissible disease. |
8.3. TGA listed respirators
To check if a respirator is suitable for HCW use, search the TGA list at Guidance on medical/surgical face masks and respirator standards - key performance aspects.
Follow these steps:
- Identify the ARTG number. This number may be listed on the product package, in the product information, or on the company website. You can also request the manufacturer or supplier to provide the ARTG number or a copy of the ARTG summary.
- Use the ARTG number to search the ARTG list TGA ARTG search function. Key words can also be searched, including product name, manufacturer, or sponsor, although this method may be less accurate than using the ARTG number as registration may be under different names.
- Review the ARTG summary to find the Global Medical Device Nomenclature (GMDN) code.
- Use the table below to confirm whether the mask or respirator is recommended for use by health care workers (HCWs) when a P2/N95 respirator is required.
Global Medical Device Nomenclature (GMDN) codes, descriptions and recommended use
| GMDN code | Description of mask or respirator | Recommended use |
|---|---|---|
| 35177 | Surgical mask – single use For use by medical personnel during surgery |
|
| 57794 | Surgical respirator – single use For use by healthcare workers during medical, surgical, dental, and isolation procedures |
|
| 57792 | Antimicrobial surgical respirator (has an antimicrobial/antiviral agent to destroy specified pathogens) For use by healthcare worker during medical, surgical, dental, and isolation procedures |
|
| 57793 | Public respirator – single use Note: Not all respirators in this category are equivalent to a P2/N95. Check the product information to confirm classification. | Respirators classified as a P2, FFP2 or N95:
Respirators not classified as a P2, FFP2 or N95:
|
64821 64822 | Public respirator (64821) – single use Public face mask (64822) – reusable For use by the general public. Suitable for community settings and industries and as an alternative to a surgical mask. |
|
Respirators that cannot be identified through a TGA search should not be used as a P2/N95 until the ARTG listing has been confirmed.
KN95 standard respirators, are different from P2/N95, and are not recommended as a P2/N95 alternative for healthcare workers or in healthcare settings.
Respirators with ear loops are not recommended by Centers for Disease Control and Prevention/National Institute for Occupational Safety and Health COVID-19: International Respirator Purchase | CDC or the Australian Institute of Occupational Hygienists Guide to Buying P2, or Equivalent, Respirators for use in the Work Environment (2020) – AIOH.
Source: Guidance on Personal Protective Equipment for Health Professionals.
8.4. COVID-19 and IPC education
For a summary of IPC education available to healthcare workers, see VICNISS – Educational Opportunities.
Training for health care workers in all settings covering the fundamentals of IPC for COVID-19 is available from the Australian Government Department of Health.
IPC training suitable for non-clinical staff is available from VICNISS - Infection Prevention and Control eLearning Modules.
Training to support organisations in meeting the requirements of the National Safety and Quality Health Service Standards, the National Safety and Quality Primary and Community Healthcare Standards and to assist in implementing effective IPC practices is available from the Australian Commission for Safety and Quality in Healthcare (ACSQH): National Hand Hygiene Initiative Learning Management System (southrock.com).
Ventilation in residential care – an education package is available at VICNISS – Ventilation in Residential Care.
8.5. Purchasing an air cleaner
An air cleaner needs to be appropriate to the size of the room and must be positioned correctly within the room. Follow manufacturer’s recommendations and seek advice from an occupational physician or IPC or ventilation professional when purchasing and positioning air cleaners.
Air cleaning device - purchasing factors
| Factor | Considerations and recommendations |
|---|---|
| Filter requirement | Air cleaners equipped with H13 HEPA filters are recommended. Air cleaners with a lower grade filter may not be as efficient in removing airborne viral particles. |
| Filter maintenance | All parts of the air cleaner will require maintenance and replacement as per the manufacturer’s instructions. Emphasis should be placed on the cleaning and maintenance of the pre-filter and HEPA filter. A HEPA-filtered vacuum cleaner should be used if manual cleaning of the pre-filter is required. Effectiveness of the air purifier could be reduced if you replace the filter with a lower quality filter. Filter changes should be undertaken outdoors where possible. Where required, appropriate Personal Protective Equipment (PPE) should be worn as per the manufacturer’s instructions. |
| Surface cleaning and disinfection | The surface of air cleaner should be treated as a frequently touched surface and cleaned as per the department’s cleaning guidelines to prevent it from becoming a source of infection. Follow the manufacturer’s instructions on how to appropriately clean device surfaces. |
| Noise levels (dB) and fan speed | Noise levels generated will depend on the fan speed and distance from the device. Each air purifier operates at a different noise level depending on the fan. Maximum recommended air purifier noise level (dB) for different environments:
For reference, a whisper is about 30 decibels (dB), normal conversation is about 60 dB, and a motorcycle engine running is about 95 dB. Two quiet air purifiers instead of one large unit is an option. |
| Costs | Costs relating to outright purchase or rental, filter replacement, energy and regular maintenance. Portable air cleaners are cost-effective, flexible solutions to reduce the risk of airborne infectious disease transmission in spaces where other ventilation and filtration modifications are impossible, or where building occupants seek additional reassurance about air quality. |
| Size | Size of the air cleaner should be appropriate to the space it will be used in. Properly sized portable air cleaners with HEPA filters can reduce in-room concentrations of airborne particles, including those carrying viral material. It may be appropriate to use more than one air purifier in a room. |
| Electrical | Measured in watts and amps. Overseas models need to be checked for compatibility with the Australian standard voltage and frequency. |
| Add-ons | Additional disinfection features such as UV, air ionisations, ozone are not required for infection prevention and control purposes. Some air purifiers use ionisers, plasma/ozone/photocatalytic oxidation/precipitators and UV technology. These are currently unproven technologies, and in some cases dangerous technologies. These chemicals and technologies can significantly degrade air quality by producing ions, ozone and oxidation. This can cause irritation, trigger asthma and/or degrade materials. |
For more information, see the University of Melbourne Guide to Air Cleaner Purchasing.
8.6. Posters
PPE
How to put on and take off your PPE - gown and gloves together
How to put on and take off your PPE - gown and gloves separately
How to put on and take off PPE - using plastic apron
How to put on and take off PPE - using coveralls
See, How to put on (don) and take off (doff) your PPE.
Caring for your skin when wearing PPE
Caring for Facial Skin Applying Dressings Under PPE
Caring for Facial Skin When Wearing a Surgical Face Mask
Caring for Facial Skin When Wearing a P2/N95 Respirator and Eye Protection
See, Caring for your skin when wearing PPE.
Face masks
See, Face masks do's and don'ts.
How to clean your personal items used at work
How to safely clean your mobile phone
How to safely clean your laptop and tablet
How to safely clean your reusable face shield
How to safely handle your drink bottle
See, How to clean your personal items used at work.
8.7 Self-assessment tools
These tools are designed as checklists and should be used as a prompt to evaluate items that need to be in place to reduce the transmission of COVID-19.
The checklists are not meant to replace detailed, site-specific policies, protocols and procedures that every service should have in place. Instead, they are intended to assist in the assessment of COVID-19 infection prevention and control policies and practices to mitigate the risk of COVID-19 transmission among staff, visitors and where applicable residents.
The tools do not provide links to financial assistance, grants, supplies procurement or other assistance schemes.
Services are responsible for understanding their eligibility and accessing these resources:
- COVID-19 Self-Assessment Tool for Residential Aged Care Facilities
- COVID-19 Self-Assessment Tool for Residential Community and Disability Services
- COVID-19 Self-Assessment Tool for Non-Residential Community and Disability Services
8.8. References
Aged care
Aged Care Quality and Safety Commission, Partnerships in care.
Cleaning and disinfecting
Australia Government, COVID-19 Information about routine environmental cleaning and disinfection in the community.
Therapeutic Goods Administration (TGA), Disinfectants for use against COVID-19 in the ARTG for legal supply in Australia.
Hand hygiene
Therapeutic Goods Administration (TGA), Hand sanitisers: Information for consumers.
Waste management
Environment Protection Authority (EPA) Victoria, Clinical and related waste – operational guidance.
Hierarchy of controls and COVID safe plans
WorkSafe Victoria, The Hierarchy of Control.
Safe Work Australia, Model Code of Practice: How to manage work health and safety risks (May 2018).
Education
VICNISS, Educational opportunities (summary of IPC education available to healthcare workers).
Australian Government Department of Health, COVID-19 infection control training module for all healthcare workers.
Australasian College of Infection Prevention and Control (ACIPC), Foundations of infection prevention and control course.
Victorian Department of Health and VICNISS, basic level Infection prevention and control eLearning modules.
Victorian Department of Health and VICNISS, Ventilation in residential care.
Infection prevention and control COVID-19 information
National Health and Medical Research Council (NHMRC), Australian Guidelines for the Prevention and Control of Infection in Healthcare.
Communicable Diseases Network Australian (CDNA), Series of National Guidelines – Coronavirus 2019 (COVID-19) guidelines.
Australian Government Department of Health and Aged Care, Infection Prevention and Control Expert Group (ICEG).
World Health Organization (WHO) guideline, Infection prevention and control during health care when COVID-19 is suspected: Interim guidance 12 July 2021.
Business Victoria, Business and work.
Victorian Department of Health, COVID-19 (Coronavirus disease 2019).
Centres for Disease Control and Prevention (CDC), Coronavirus Disease 2019 (COVID-19).
Therapeutic Goods Administration (TGA)
Australian Health Protection Principal Committee (AHPPC)
Clinical Excellence Commission, COVID-19 Infection Prevention and Control Manual.
National Library of Medicine, A Paradigm Shift to Align Transmission Routes With Mechanisms - PubMed (nih.gov).
At-risk workers
Royal Australia and New Zealand College of Obstetricians and Gynaecologists (RANZCOG), COVID-19 and pregnant health care workers and other at-risk workers.
Animals and pets
Australian Veterinary Association (ava.com.au), Coronavirus.
Centers for Disease Control and Prevention (CDC), Information about COVID-19, Pets, and Other Animals.
Respiratory Protection Program
Victorian Department of Health, Victorian Respiratory Protection Program.
Ventilation and buildings
Australian Commission on Safety and Quality in Health Care, Optimising ventilation for infection prevention and control in healthcare settings.
Better Health Channel, Ventilation.
Victorian Health Building Authority (VHBA), HVAC system strategies to airborne infectious outbreaks.
Victorian Health Building Authority, Technical guidelines.
Victorian Department of Health, Maintenance standards for critical areas in Victorian health facilities.
Australasian Health Facility Guidelines (AusHFG), Health Infrastructure Alliance.